BIOCHEMISTRY
AND PATHOBIOCHEMISTRY OF BLOOD. RESPIRATORY FUNCTION OF ERYTHROCYTES. PATHOLOGICAL
FORMS OF HEMOGLOBIN. ACID-BASE STATE OF BLOOD. BIOCHEMICAL COMPOSITION OF BLOOD IN NORM
AND PATHOLOGY: ACUTE PHASE PROTEINS, ENZYMES OF BLOOD PLASMA. RESIDUAL
NITROGEN. BIOCHEMICAL FUNCTIONS OF LIVER. METABOLISM
OF PORPHYRINS: METABOLISM OF BILE PIGMENTS, BIOCHEMISTRY OF JAUNDICES. BIOTRANSFORMATION OF
XENOBIOTICS AND ENDOGENOUS TOXINS IN THE LIVER: MICROSOMAL OXIDATION, CYTOCHROME Р-450. URINE FORMATION, FUNCTION OF KIDNEY. PHYSICAL AND CHEMICAL PROPERTIES AND
CHEMICAL COMPOSITION OF NORMAL URINE.
PATHOBIOCHEMISTRY OF KIDNEY. PATHOLOGICAL COMPONENTS OF URINE.
Blood
is a liquid tissue. Suspended in the watery plasma are seven types of cells and
cell fragments.
• red blood cells (RBCs) or erythrocytes
• platelets or thrombocytes
• five kinds of white blood cells (WBCs) or
leukocytes
Three kinds of granulocytes
neutrophils
eosinophils
basophils
Two kinds of leukocytes without granules in
their cytoplasm
lymphocytes
monocytes
If
one takes a sample of blood, treats it with an agent to prevent clotting, and
spins it in a centrifuge,
• the red cells settle to the bottom
• the white cells settle on top of them forming
the "buffy coat".
The
fraction occupied by the red cells is called the hematocrit. Normally it is
approximately 45%. Values much lower than this are a sign of anemia
|
.
|

|
Biological functions of the blood
The blood is the most specialized fluid tissue which
circulates in vascular system and together with lymph and intercellular space
compounds an internal environment of an organism.
The blood
executes such functions:
1. Transport of gases – oxygen from lungs is carried to
tissues and carbon dioxide from tissues to lungs.
2. Transport of
nutrients to all cells of organism (glucose, amino acids, fatty acids,
vitamins, ketone bodies, trace substances and others). Substances such as urea,
uric acid, bilirubin and creatinine are taken away from the different organs
for ultimate excretion.
3. Regulatory or
hormonal function – hormones are secreted in to blood and they are transported
by blood to their target cells.
4. Thermoregulation function - an exchange of heat
between tissues and blood.
5. Osmotic function- sustains osmotic pressure in
vessels.
6. Protective function- by the phagocytic action of
leucocytes and by the actions of antibodies, the blood provides the most
important defense mechanism.
7. Detoxification function - neutralization of toxic
substances which is connected with their decomposition by the help of blood
enzymes.
Blood
performs two major functions:
- transport through the body of
- oxygen and carbon dioxide
- food molecules (glucose, lipids, amino acids)
- ions (e.g., Na+, Ca2+, HCO3−)
- wastes (e.g., urea)
- hormones
- heat
- defense of
the body against infections and other foreign materials. All the WBCs participate in
these defenses.
The formation of blood cells (cell types and acronyms are
defined below)
All the various types of blood cells
·
are produced in the bone marrow
(some 1011 of them each day in an adult human!).
·
arise from a single type of cell
called a hematopoietic stem cell — an "adult" multipotent stem
cell.
These stem cells
- are very rare (only about one in
10,000 bone marrow cells);
- are attached (probably by adherens
junctions) to osteoblasts lining the inner surface of bone cavities;
- express a cell-surface protein
designated CD34;
- produce, by mitosis, two kinds
of progeny:
- more stem cells (A mouse
that has had all its blood stem cells killed by a lethal dose of
radiation can be saved by the injection of a single living stem cell!).
- cells that begin to
differentiate along the paths leading to the various kinds of blood
cells.
Which
path is taken is regulated by
- the need for more of that type
of blood cell which is, in turn, controlled by appropriate cytokines and/or hormones.
Examples:
- Interleukin-7 (IL-7) is the major cytokine in stimulating bone marrow
stem cells to start down the path leading to the various lymphocytes (mostly B cells and T cells).
- Erythropoietin (EPO), produced by the kidneys, enhances the production of red
blood cells (RBCs).
- Thrombopoietin (TPO), assisted by Interleukin-11 (IL-11),
stimulates the production of megakaryocytes. Their fragmentation produces platelets.
- Granulocyte-macrophage
colony-stimulating factor (GM-CSF), as its
name suggests, sends cells down the path leading to both those cell types.
In due course, one path or the other is taken.
- Under the influence of granulocyte
colony-stimulating factor (G-CSF), they differentiate into neutrophils.
- Further stimulated by
interleukin-5 (IL-5) they develop into eosinophils.
o
Interleukin-3 (IL-3)
participates in the differentiation of most of the white blood cells but plays
a particularly prominent role in the formation of basophils
(responsible for some allergies).
o
Stimulated by macrophage
colony-stimulating factor (M-CSF) the granulocyte/macrophage
progenitor cells differentiate into monocytes,
macrophages, and dendritic cells
(DCs).
Biological
chemistry of blood cells
Two types of
blood cells can be distinguished - white and red blood cells. White blood cells
are called leucocytes. Their quantity in adult is 4-9 x 109/L.
Red blood cells are called erythrocytes. Their quantity
in peripheral blood is 4,5-5 x 1012/L. Besides that, there are also
thrombocytes or platelets in blood.
White
Blood Cells (leukocytes)
Leucocytes (white blood cells) protect an organism from
microorganisms, viruses and foreign substances, that provides the immune status
of an organism.
- are much
less numerous than red (the ratio between the two is around 1:700),
- have nuclei,
- participate
in protecting the body from infection,
- consist
of lymphocytes and monocytes with relatively clear
cytoplasm, and three types of granulocytes, whose cytoplasm is
filled with granules.
Leucocytes are divided into two groups: Granulocytes and
agranulocytes. Granulocytes consist of neutrophils, eosinophils and basophils.
Agranulocytes consist of monocytes and lymphocytes.
http://www.youtube.com/watch?v=8ytkFqAMoa8
http://www.youtube.com/watch?v=ce0Xndms1bc
Neutrophils
Neutrophils comprise of 60-70 % from all leucocytes.
Their main function is to protect organisms from microorganisms and viruses.
Neutrophils have segmented nucleus, endoplasmic reticulum (underdeveloped)
which does not contain ribosomes, insufficient amount of mitochondria,
well-developed Golgi apparatus and hundreds of different vesicles which contain
peroxidases and hydrolases. Optimum condition for their activity is acidic pH. There
are also small vesicles which contain alkaline phosphatases, lysozymes, lactopherins and proteins
of cationic origin.
Glucose is the main source of
energy for neutrophils. It is directly utilized or converted into glycogen. 90
% of energy is formed in glycolysis, a small amount of glucose is converted in
pentosophosphate pathway. Activation of proteolysis during phagocytosis as well
as reduction of phosphatidic acid and phosphoglycerols are also observed. The
englobement is accompanied by intensifying of a glycolysis and pentosophosphate
pathway. But especially intensity of absorption of oxygen for neutrophils -
so-called flashout of respiration grows. Absorbed oxygen is spent for formation
of its fissile forms that is carried out with participation enzymes:
1. NADP*Н -OXYDASE catalyzes formation of super oxide anion
2. An enzyme NADH- OXYDASE is responsible for formation of hydrogen peroxide
3. Мyeloperoxydase
catalyzes formation of hypochloric acid from chloride and hydrogen peroxide
Neutrophils are motile phagocyte cells that play
a key role in acute inflammation. When bacteria enter tissues, a number of
phenomena occur that are collectively known as acute inflammatory response.
When neutrophils and other phagocyte cells engulf bacteria, they exhibit a
rapid increase in oxygen consumption known as the respiratory burst. This
phenomenon reflects the rapid utilization of oxygen (following a lag of 15-60
seconds) and production from it of large amounts of reactive derivates, such as
O2-, H2O2, OH. and OCl- (hypochlorite ion). Some of these products
are potent microbicidal agents. The electron transport chain system responsible
for the respiratory burst contains several components, including a flavoprotein
NADPH:O2-oxidoreductase (often called NADPH-oxidase) and a b-type
cytochrome.
The most abundant of the WBCs. This photomicrograph
shows a single neutrophil surrounded by red blood cells.
Neutrophils squeeze through the capillary walls and
into infected tissue where they kill the invaders (e.g., bacteria) and then
engulf the remnants by phagocytosis.
This is a never-ending task, even in healthy people:
Our throat, nasal passages, and colon harbor vast numbers of bacteria. Most of
these are commensals, and do us no harm. But that is because neutrophils keep
them in check.
However,
- heavy doses of radiation
- chemotherapy
- and many
other forms of stress
can
reduce the numbers of neutrophils so that formerly harmless bacteria begin to
proliferate. The resulting opportunistic infection can be
life-threatening.
http://www.youtube.com/watch?v=EpC6G_DGqkI&feature=related
Some important enzymes and proteins
of neutrophilis.
Myeloperoxidase
(MPO). Catalyzed following reaction:
H2O2 + X-(halide)
+ H+®
HOX + H2O (where X- = Cl-, Br-, I-
or SCN-; HOX=hypochlorous acid)
HOCl, the active ingredient of household liquid
bleach, is a powerful oxidant and is highly microbicidial. When applied to
normal tissues, its potential for causing damage is diminished because it
reacts with primary or secondary amines present in neutrophils and tissues to
produce various nitrogen-chlorine (N-Cl) derivates; these chloramines are also
oxidants, although less powerful than HOCl, and act as microbicidial agents (eg,
in sterilizing wounds) without causing tissue damage. Responsible for the green
color of pus.
NADPH-oxidase.
2O2 + NADPH ®
2O2- + NADP + H+
Key component of the respiratory burst.
Deficiency may be observed in chronic granulomatous disease.
Lysozyme.
Hydrolyzes link between N-acetylmuramic acid and
N-acetyl-D-glucosamine found in certain bacterial cell walls. Abundant in
macrophages.
Defensins.
Basic antibiotic peptides of 29-33 amino acids.
Apparently kill bacteria by causing membrane damage.
Lactoferrin.
Iron-binding protein. May inhibit growth of
certain bacteria by binding iron and may be involved in regulation of
proliferation of myeloid cells.
Neutrophils contain a number of proteinases
(elastase, collagenase, gelatinase, cathepsin G, plasminogen activator) that
can hydrolyze elastin, various types of collagens, and other proteins present
in the extracellular matrix. Such enzymatic action, if allowed to proceed
unopposed, can result in serious damage to tissues. Most of these proteinases
are lysosomal enzymes and exist mainly as inactive precursors in normal
neutrophils. Small amounts of these enzymes are released into normal tissues,
with the amounts increasing markedly during inflammation. The activities of
elastase and other proteinases are normally kept in check by a number of
antiproteinases (a1-Antiproteinase,
a2-Macroglobulin,
Secretory leukoproteinase inhibitor, a1-Antichymotrypsin,
Plasminogen activator inhibitor-1, Tissue inhibitor of metalloproteinase) present
in plasma and the extracellular fluid.
Basophiles
Basophiles make up 1-5% of all blood leukocytes. They
are actively formed in the bone marrow
during allergy. Basophiles take part in
the allergic reactions, in the blood coagulation and intravascular
lipolysis. They have the protein synthesis mechanism, which works due to the
biological oxidation energy . They synthesize the mediators of allergic
reactions – histamine and serotonin, which during allergy cause local
inflammation. Heparin, which is formed in the basophiles, prevents the blood
coagulation and activates intravascular lipoprotein lipase, which splits triacylglycerin.
The number of basophils also increases during
infection. Basophils leave the blood and accumulate at the site of infection or
other inflammation. There they discharge the contents of their granules,
releasing a variety of mediators such as:
which
increase the blood flow to the area and in other ways add to the inflammatory
process. The mediators released by basophils also play an important part in
some allergic responses such as
Eosinophiles
They make up 3-6% of all leukocytes. Eosinophiles as
well as neutrophiles defend the cells from microorganisms, they contain
myeloperoxidase, lysosomal hydrolases. About the relations of eosinophiles with
testifies the growth of their amount during the sensitization of organism, i.e.
during bronchial asthma, helminthiasis. They are able to pile and splits
histamine, “to dissolve” thrombus with the participation of plasminogen and
bradykinin-kininase.
Monocytes
They are formed in the bone marrow. They make up 4-8% of all leukocytes.
According to the function they are called macrophages. Tissue macrophages
derive from blood monocytes. Depending on their position they are called: in
the liver – reticuloendotheliocytes, in the lungs - alveolar macrophages, in
the intermediate substance of connective tissue – histocytes etc. Monocytes are
characterized by a wide set of lysosomal
enzymes with the optimum activity in the acidic condition. The major
functions of monocytes and macrophages are endocytosis and phagocytosis.
Lymphocytes
The amount – 20-25%, are formed in
the lymphoid tissue or thymus, play important role in the formation of humoral
and cellular immunity. Lymphocytes have powerful system of synthesis of
antibody proteins, energy is majorily pertained due to glycolysis, rarely – by
aerobic way.
http://www.youtube.com/watch?v=cD_uAGPBfQQ&feature=related
There
are several kinds of lymphocytes (although they all look alike under the microscope),
each with different functions to perform . The most common types of lymphocytes
are
- B lymphocytes ("B cells"). These are responsible for making
antibodies.
- T
lymphocytes ("T cells"). There are several
subsets of these:
Although bone marrow is the ultimate source of
lymphocytes, the lymphocytes that will become T cells migrate from the bone
marrow to the thymus where they
mature. Both B cells and T cells also take up residence in lymph nodes, the
spleen and other tissues where they
- encounter antigens;
- continue
to divide by mitosis;
- mature
into fully functional cells.
Monocytes
Monocytes
leave the blood and become macrophages and dendritic cells.
This scanning electron micrograph (courtesy of Drs. Jan
M. Orenstein and Emma Shelton) shows a single macrophage surrounded by several
lymphocytes.
Macrophages
are large, phagocytic cells that engulf
- foreign
material (antigens) that enter the body
- dead and
dying cells of the body.
Thrombocytes
(blood platelets)
Platelets
are cell fragments produced from megakaryocytes.
Blood normally contains 150,000–350,000 per microliter
(µl) or cubic millimeter (mm3). This number is normally maintained
by a homeostatic (negative-feedback) mechanism .
The amount – less than 1%, they play
the main role in the process of hemostasis. They are formed as a result of
disintegration of megakaryocytes in the bone
marrow. Their –life-time is 7-9 days. In spite of the fact that
thrombocytes have no nucleus, they are able to perform practically all
functions of the cell, besides DNA synthesis.
If this value should drop much below 50,000/µl, there
is a danger of uncontrolled bleeding because of the essential role that
platelets have in blood clotting.
Some causes:
- certain
drugs and herbal remedies;
- autoimmunity.
When blood vessels are cut or damaged, the loss of
blood from the system must be stopped before shock and possible death occur. This is accomplished by
solidification of the blood, a process called coagulation or clotting.
A blood clot consists of
- a plug
of platelets enmeshed in a
- network
of insoluble fibrin molecules.
Red Blood Cells
(erythrocytes)
The
most numerous type in the blood.
- Women
average about 4.8 million of these cells per cubic millimeter (mm3;
which is the same as a microliter [µl]) of blood.
- Men
average about 5.4 x 106 per µl.
- These
values can vary over quite a range depending on such factors as health and
altitude. (Peruvians living at 18,000 feet may
have as many as 8.3 x 106 RBCs per µl.)
RBC
precursors mature in the bone marrow closely attached to a macrophage.
- They
manufacture hemoglobin until it accounts for some 90% of the dry weight of
the cell.
- The
nucleus is squeezed out of the cell and is ingested by the macrophage.
- No-longer-needed
proteins are expelled from the cell in vesicles called exosomes.
Human blood contains 25 trillion of erythrocytes.
Their main function – transportation of O2 and CO2 – they
perform due to the fact that they contain 34% of hemoglobin, and per dry cells
mass – 95%. The total amount of
hemoglobin in the blood equals 130-160 g/l. In the process of erythropoesis the
preceding cells decrease their size. Their nuclei at the end of the process are
ruined and pushed out of the cells. 90% of glucose in the erythrocytes is
decomposed in the process of glycolysis and 10% - by pentose-phosphate way.
There are noted congenital defects of enzymes of these metabolic ways of
erythrocytes. During this are usually observed hemolytic anemia and other
structural and functional erythrocytes’ affections.
This scanning electron micrograph (courtesy of Dr.
Marion J. Barnhart) shows the characteristic biconcave shape of red blood
cells.
Thus RBCs are terminally differentiated; that is, they can never divide.
They live about 120 days and then are ingested by phagocytic cells in the liver
and spleen. Most of the iron in their hemoglobin is reclaimed for reuse. The
remainder of the heme portion of the molecule is degraded into bile pigments and excreted by the liver. Some 3 million RBCs die
and are scavenged by the liver each second.
Red
blood cells are responsible for the transport of oxygen and carbon
dioxide.
Oxygen Transport
In
adult humans the hemoglobin (Hb) molecule
- consists of four polypeptides:
o
two alpha (α) chains
of 141 amino acids and
o
two beta (β) chains
of 146 amino acids
- Each of these is attached the prosthetic
group heme.
- There is
one atom of iron at the center of each heme.
- One
molecule of oxygen can bind to each heme.
http://www.youtube.com/watch?v=WXOBJEXxNEo&feature=related
The
reaction is reversible.
- Under
the conditions of lower temperature, higher pH, and increased oxygen
pressure in the capillaries of the lungs, the reaction proceeds to the
right. The purple-red deoxygenated hemoglobin of the venous blood becomes
the bright-red oxyhemoglobin of the arterial blood.
- Under
the conditions of higher temperature, lower pH, and lower oxygen pressure
in the tissues, the reverse reaction is promoted and oxyhemoglobin gives
up its oxygen.
Carbon
Dioxide Transport
Carbon
dioxide (CO2) combines with water forming carbonic acid, which
dissociates into a hydrogen ion (H+) and a bicarbonate ions
:
CO2
+ H2O ↔ H2CO3 ↔ H+ +
HCO3−
95%
of the CO2 generated in the tissues is carried in the red blood
cells:
Only
about 5% of the CO2 generated in the tissues dissolves directly in
the plasma. (A good thing, too: if all the CO2 we make were carried
this way, the pH of the blood would drop from its normal 7.4 to an
instantly-fatal 4.5!)
When
the red cells reach the lungs, these reactions are reversed and CO2
is released to the air of the alveoli.
Anemia
is a shortage of
Anemia
has many causes. One of the most common is an inadequate intake of iron in the
diet.
Red
blood cells have surface antigens that differ between people and that create
the so-called blood groups such as the ABO system and the Rh
system.
An
Essay on Hemoglobin Structure and Function:
Figure 1 is a model of human
deoxyhemoglobin. It was created in RasMol version 2.6 by Roger Sayle
using the pdb coordinates from the pdb file 4hhb. The 3D coordinates were
determed from x-ray crystallography by Fermi, G., Perutz, M. F., Shaanan, B.,
Fourme, R.: The crystal structure of human deoxyhaemoglobin at 1.74 A
resolution. J Mol Biol 175 pp. 159 (1984)
Hemoglobin
is the protein that carries oxygen from the lungs to the tissues and carries
carbon dioxide from the tissues back to the lungs. In order to function most
efficiently, hemoglobin needs to bind to oxygen tightly in the oxygen-rich
atmosphere of the lungs and be able to release oxygen rapidly in the relatively
oxygen-poor environment of the tissues. It does this in a most elegant and
intricately coordinated way. The story of hemoglobin is the prototype example
of the relationship between structure and function of a protein molecule.
Hemoglobin
Structure
A
hemoglobin molecule consists of four polypeptide chains: two alpha chains, each
with 141 amino acids and two beta chains, each with 146 amino acids. The
protein portion of each of these chains is called "globin". The a and
b globin chains are very similar in structure. In this case, a and b refer to
the two types of globin. Students often confuse this with the concept of a
helix and b sheet secondary structures. But, in fact, both the a and b globin
chains contain primarily a helix secondary structure with no b sheets.
Figure 2 is a close up view of one
of the heme groups of the human a chain from dexoyhemoglobin. In this
view, the iron is coordinated by a histidine side chain from amino acid 87
(shown in green.)
Each
a or b globin chain folds into 8 a helical segments (A-H) which, in turn, fold
to form globular tertiary structures that look roughly like sub-microscopic
kidney beans. The folded helices form a pocket that holds the working part of
each chain, the heme.
http://www.youtube.com/watch?v=eor6EK_JP40
A
heme group is a flat ring molecule containing carbon, nitrogen and hydrogen
atoms, with a single Fe2+ ion at the center. Without the iron, the
ring is called a porphyrin. In a heme molecule, the iron is held within the
flat plane by four nitrogen ligands from the porphyrin ring. The iron ion makes
a fifth bond to a histidine side chain from one of the helices that form the
heme pocket. This fifth coordination bond is to histidine 87 in the human a
chain and histidine 92 in the human b chain. Both histidine residues are part
of the F helix in each globin chain. t
The Bohr
Effect
The
ability of hemoglobin to release oxygen, is affected by pH, CO2 and
by the differences in the oxygen-rich environment of the lungs and the
oxygen-poor environment of the tissues. The pH in the tissues is considerably lower
(more acidic) than in the lungs. Protons are generated from the reaction
between carbon dioxide and water to form bicarbonate:
CO2
+ H20 -----------------> HCO3- + H+
This
increased acidity serves a twofold purpose. First, protons lower the affinity
of hemoglobin for oxygen, allowing easier release into the tissues. As all four
oxygens are released, hemoglobin binds to two protons. This helps to maintain
equilibrium towards the right side of the equation. This is known as the Bohr
effect, and is vital in the removal of carbon dioxide as waste because CO2
is insoluble in the bloodstream. The bicarbonate ion is much more soluble, and
can thereby be transported back to the lungs after being bound to hemoglobin.
If hemoglobin couldn’t absorb the excess protons, the equilibrium would shift
to the left, and carbon dioxide couldn’t be removed.
In
the lungs, this effect works in the reverse direction. In the presence of the
high oxygen concentration in the lungs, the proton affinity decreases. As
protons are shed, the reaction is driven to the left, and CO2 forms
as an insoluble gas to be expelled from the lungs. The proton poor hemoglobin
now has a greater affinity for oxygen, and the cycle continues.
Haemoglobin or hemoglobin
(frequently abbreviated as Hb or Hgb) is the iron-containing
oxygen-transport
metalloprotein
in the red
blood cells of the blood
in vertebrates
and other animals; in mammals
the protein makes up about 97% of the red cell’s dry content, and around 35% of
the total content including water. Hemoglobin transports oxygen from the lungs
or gills
to the rest of the body, such as to the muscles,
where it releases the oxygen load. Hemoglobin also has a variety of other
gas-transport and effect-modulation duties, which vary from species to species,
and which in invertebrates may be quite diverse.
The
name hemoglobin is the concatenation of heme and globin,
reflecting the fact that each subunit
of hemoglobin is a globular
protein with an embedded heme
(or haem) group; each heme group contains an iron
atom, and this is responsible for the binding of oxygen. The most common type
of hemoglobin in mammals contains four such subunits, each with one heme group.
Mutations
in the genes
for the hemoglobin protein in humans result in a group of hereditary
diseases termed the hemoglobinopathies,
the most common members of which are sickle-cell
disease and thalassemia.
Historically in human medicine, the hemoglobinopathy of sickle-cell
disease was the first disease to be understood in its mechanism of
dysfunction, completely down to the molecular level. However, not all of such
mutations produce disease states, and are formally recognized as hemoglobin
variants (not diseases).[1][2]
Hemoglobin
(Hb) is synthesized in a complex series of steps. The heme
portion is sythesized in both the the mitochondria
and cytosol
of the immature red blood cell, while the globin
protein portions of the molecule are sythesized by ribosomes in the cytosol [3].
Production of Hb continues in the cell throughout its early development from
the proerythroblast
to the reticulocyte
in the bone
marrow. At this point, the nucleus is lost in mammals, but not in
birds and many other species. Even after the loss of the nucleus in mammals,
however, residual ribosomal RNA allows further synthesis of Hb until the
reticulocyte loses its RNA soon after entering the vasculature (this
hemoglobin-synthetic RNA in fact gives the reticulocyte
its reticulated appearance and name).
The
empirical chemical formula of the most common human hemoglobin is C2952H4664N812O832S8Fe4,
but as noted above, hemoglobins vary widely across species, and even (through
common mutations) slightly among subgroups of humans.
In
humans, the hemoglobin molecule
is an assembly of four globular
protein subunits. Each subunit
is composed of a protein
chain tightly associated with a non-protein heme
group. Each protein chain arranges into a set of alpha-helix
structural segments connected together in a globin
fold arrangement, so called because this arrangement is the same
folding motif used in other heme/globin proteins such as myoglobin.[4][5]
This folding pattern contains a pocket which strongly binds the heme group.
A
heme group consists of an iron
(Fe) atom held in a heterocyclic
ring, known as a porphyrin.
The iron atom, which is the site of oxygen binding, bonds with the four nitrogens
in the center of the ring, which all lie in one plane. The iron is also bound
strongly to the globular protein via the imidazole
ring of a histidine
residue below the porphyrin ring. A sixth position can reversibly bind oxygen,
completing the octahedral group of six ligands. Oxygen binds in an "end-on
bent" geometry where one oxygen atom binds Fe and the other protrudes at
an angle. When oxygen is not bound, a very weakly bonded water molecule fills
the site, forming a distorted octahedron.
The
iron atom may either be in the Fe2+ or Fe3+ state, but
ferrihemoglobin (methemoglobin)
(Fe3+) cannot bind oxygen. In binding, oxygen temporarily oxidizes
Fe to (Fe3+), so iron must exist in the +2 oxidation state in order
to bind oxygen. The body reactivates hemoglobin found in the inactive (Fe3+)
state by reducing the iron center.
In
adult humans, the most common hemoglobin type is a tetramer
(which contains 4 subunit proteins) called hemoglobin A, consisting of
two α and two β subunits non-covalently bound, each made of 141 and
146 amino acid residues, respectively. This is denoted as α2β2.
The subunits are structurally similar and about the same size. Each subunit has
a molecular weight of about 17,000 daltons,
for a total molecular
weight of the tetramer of about 68,000 daltons. Hemoglobin A is
the most intensively studied of the hemoglobin molecules.
The
four polypeptide
chains are bound to each other by salt
bridges, hydrogen
bonds, and hydrophobic
interactions. There are two kinds of contacts between the α and
β chains: α1β1 and α1β2.
Oxyhemoglobin is formed during respiration when oxygen
binds to the heme
component of the protein hemoglobin in red blood cells. This process occurs in
the pulmonary capillaries adjacent to the alveoli
of the lungs.
The oxygen then travels through the blood stream to be dropped off at cells
where it is utilized in aerobic glycolysis
and in the production of ATP
by the process of oxidative
phosphorylation. It doesn't however help to counteract a decrease in
blood pH. Ventilation,
or breathing, may reverse this condition by removal of carbon dioxide, thus
causing a shift up in pH.[6]
Deoxyhemoglobin is the form of hemoglobin without the bound oxygen.
The absorption
spectra of oxyhemoglobin and deoxyhemoglobin differ. The
oxyhemoglobine has significantly lower absorption of the 660 nm wavelength
than deoxyhemoglobin, while at 940 nm its absorption is slightly higher.
This difference is used for measurement of the amount of oxygen in patient's
blood by an instrument called pulse
oximeter.
The
oxidation state of iron in hemoglobin is always +2. It does not change when
oxygen binds to the deoxy- form.
Assigning
oxygenated hemoglobin's oxidation state is difficult because oxyhemoglobin is
diamagnetic (no net unpaired electrons), but the low-energy electron
configurations in both oxygen and iron are paramagnetic. Triplet oxygen, the
lowest energy oxygen species, has two unpaired electrons in antibonding π*
molecular orbitals. Iron(II) tends to be in a high-spin configuration where
unpaired electrons exist in eg antibonding orbitals. Iron(III) has an
odd number of electrons and necessarily has unpaired electrons. All of these
molecules are paramagnetic (have unpaired electrons), not diamagnetic, so an
unintuitive distribution of electrons must exist to induce diamagnetism.
The
three logical possibilities are:
1)
Low-spin Fe2+ binds to high-energy singlet oxygen. Both low-spin
iron and singlet oxygen are diamagnetic.
2)
High-spin Fe3+ binds to .O2- (the superoxide
ion) and antiferromagnetism oppositely aligns the two unpaired electrons,
giving diamagnetic properties.
3)
Low-spin Fe4+ binds to O22-. Both are
diamagnetic.
X-ray
photoelectron spectroscopy suggests that iron has an oxidation state
of approximately 3.2 and infrared
stretching frequencies of the O-O bond suggests a bond length
fitting with superoxide. The correct oxidation state of iron is thus the +3
state with oxygen in the -1 state. The diamagnetism in this configuration
arises from the unpaired electron on superoxide aligning antiferromagnetically
in the opposite direction from the unpaired electron on iron. The second choice
being correct is not surprising because singlet oxygen and large separations of
charge are both unfavorably high-energy states. Iron's shift to a higher
oxidation state decreases the atom's size and allows it into the plane of the
porphyrin ring, pulling on the coordinated histidine residue and initiating the
allosteric changes seen in the globulins. The assignment of oxidation state,
however, is only a formalism so all three models may contribute to some small
degree.
Early
postulates by bioinorganic chemists claimed that possibility (1) (above) was
correct and that iron should exist in oxidation state II (indeed iron oxidation
state III as methemoglobin, when not accompanied by superoxide .O2-
to "hold" the oxidation electron, is incapable of binding O2).
The iron chemistry in this model was elegant, but the presence of singlet
oxygen was never explained. It was argued that the binding of an oxygen
molecule placed high-spin iron(II) in an octahedral field of strong-field
ligands; this change in field would increase the crystal
field splitting energy, causing iron's electrons to pair into the
diamagnetic low-spin configuration.
Binding
and release of ligands induces a conformational (structural) change in
hemoglobin. Here, the binding and release of oxygen illustrates the structural
differences between oxy- and deoxyhemoglobin, respectively. Only one of the
four heme groups is shown.
As
discussed above, when oxygen binds to the iron center it causes contraction of
the iron atom, and causes it to move back into the center of the porphyrin ring
plane (see moving diagram). At the same time, the porphyrin ring plane itself
is pushed away from the oxygen and toward the imidizole side chain of the
histidine residue interacting at the other pole of the iron. The interaction
here forces the ring plane sideways toward the outside of the tetramer, and
also induces a strain on the protein helix containing the histidine, as it
moves nearer the iron. This causes a tug on this peptide strand which tends to
open up heme units in the remainder of the molecule, so that there is more room
for oxygen to bind at their heme sites.
In
the tetrameric form of normal adult hemoglobin, the binding of oxygen is thus a
cooperative
process. The binding affinity of hemoglobin for oxygen is increased by the
oxygen saturation of the molecule, with the first oxygens bound influencing the
shape of the binding sites for the next oxygens, in a way favorable for
binding. This positive cooperative binding is achieved through steric
conformational changes of the hemoglobin protein complex as discussed above,
i.e. when one subunit protein in hemoglobin becomes oxygenated, this induces a
conformational or structural change in the whole complex, causing the other
subunits to gain an increased affinity for oxygen. As a consequence, the oxygen
binding curve of hemoglobin is sigmoidal,
or S-shaped, as opposed to the normal hyperbolic
curve associated with noncooperative binding.
Hemoglobin's
oxygen-binding capacity is decreased in the presence of carbon
monoxide because both gases compete for the same binding sites on
hemoglobin, carbon monoxide binding preferentially in place of oxygen. Carbon dioxide
occupies a different binding site on the hemoglobin. Through the enzyme carbonic
anhydrase, carbon dioxide reacts with water to give carbonic
acid, which decomposes into bicarbonate
and protons:
CO2
+ H2O → H2CO3 → HCO3-
+ H+
The
sigmoidal shape of hemoglobin's oxygen-dissociation curve results from cooperative
binding of oxygen to hemoglobin.
Hence
blood with high carbon dioxide levels is also lower in pH
(more acidic).
Hemoglobin can bind protons
and carbon dioxide which causes a conformational change in the protein and
facilitates the release of oxygen. Protons bind at various places along the
protein, and carbon dioxide binds at the alpha-amino
group forming carbamate.
Conversely, when the carbon dioxide levels in the blood decrease (i.e., in the
lung capillaries), carbon dioxide and protons are released from hemoglobin,
increasing the oxygen affinity of the protein. This control of hemoglobin's
affinity for oxygen by the binding and release of carbon dioxide and acid, is
known as the Bohr
effect.
The
binding of oxygen is affected by molecules such as carbon
monoxide (CO) (for example from tobacco
smoking, cars and furnaces). CO competes with oxygen at the heme
binding site. Hemoglobin binding affinity for CO is 200 times greater than its
affinity for oxygen, meaning that small amounts of CO dramatically reduces
hemoglobin's ability to transport oxygen. When hemoglobin combines with CO, it
forms a very bright red compound called carboxyhemoglobin.
When inspired air contains CO levels as low as 0.02%, headache and nausea
occur; if the CO concentration is increased to 0.1%, unconsciousness will
follow. In heavy smokers, up to 20% of the oxygen-active sites can be blocked
by CO.
In
similar fashion, hemoglobin also has competitive binding affinity for cyanide
(CN-), sulfur
monoxide (SO), nitrogen
dioxide (NO2), and sulfide (S2-), including hydrogen
sulfide (H2S). All of these bind to iron in heme without
changing its oxidation state, but they nevertheless inhibit oxygen-binding,
causing grave toxicity.
The
iron atom in the heme group must be in the Fe2+ oxidation state to
support oxygen and other gases' binding and transport. Oxidation to Fe3+
state converts hemoglobin into hemiglobin or methemoglobin
(pronounced "MET-hemoglobin"), which cannot bind oxygen. Hemoglobin
in normal red blood cells is protected by a reduction system to keep this from
happening. Nitrogen dioxide and nitrous
oxide are capable of converting a small fraction of hemoglobin to
methemoglobin, however this is not usually of medical importance (nitrogen
dioxide is poisonous by other mechanisms, and nitrous oxide is routinely used
in surgical anesthesia in most people without undue methemoglobin buildup).
In
people acclimated to high altitudes, the concentration of 2,3-bisphosphoglycerate
(2,3-BPG) in the blood is increased, which allows these individuals to deliver
a larger amount of oxygen to tissues under conditions of lower oxygen tension.
This phenomenon, where molecule Y affects the binding of molecule X to a
transport molecule Z, is called a heterotropic allosteric
effect.
A
variant hemoglobin, called fetal
hemoglobin (HbF, α2γ2), is found in
the developing fetus,
and binds oxygen with greater affinity than adult hemoglobin. This means that
the oxygen binding curve for fetal hemoglobin is left-shifted (i.e., a higher
percentage of hemoglobin has oxygen bound to it at lower oxygen tension), in
comparison to that of adult hemoglobin. As a result, fetal blood in the placenta
is able to take oxygen from maternal blood.
Hemoglobin
also carries nitric
oxide in the globin part of the molecule. This improves oxygen
delivery in the periphery and contributes to the control of respiration. NO
binds reversibly to a specific cystein residue in globin; the binding depends
on the state (R or T) of the hemoglobin. The resulting S-nitrosylated
hemoglobin influences various NO-related activities such as the control of
vascular resistance, blood pressure and respiration. NO is released not in the
cytoplasm of erythrocytes but is transported by an anion exchanger called AE1
out of them.[7]
When
red
cells reach the end of their life due to aging or defects, they are
broken down, the hemoglobin molecule is broken up and the iron gets recycled.
When the porphyrin ring is broken up, the fragments are normally secreted in
the bile
by the liver.
This process also produces one molecule of carbon
monoxide for every molecule of heme degraded [4];
this is one of the few natural sources of carbon
monoxide production in the human body, and is responsible for the
normal blood levels of carbon monoxide even in people breathing pure air. The
other major final product of heme degradation is bilirubin.
Increased levels of this chemical are detected in the blood if red cells are
being destroyed more rapidly than usual. Improperly degraded hemoglobin protein
or hemoglobin that has been released from the blood cells too rapidly can clog
small blood vessels, especially the delicate blood filtering vessels of the kidneys,
causing kidney damage
Decrease
of hemoglobin, with or without an absolute decrease of red
blood cells, leads to symptoms of anemia.
Anemia has many different causes, although iron
deficiency and its resultant iron
deficiency anemia are the most common causes in the Western world.
As absence of iron decreases heme
synthesis, red blood cells in iron deficiency anemia are hypochromic (lacking
the red hemoglobin pigment) and microcytic (smaller than normal). Other
anemias are rarer. In hemolysis
(accelerated breakdown of red blood cells), associated jaundice
is caused by the hemoglobin metabolite bilirubin,
and the circulating hemoglobin can cause renal
failure.
Some
mutations in the globin chain are associated with the hemoglobinopathies,
such as sickle-cell
disease and thalassemia.
Other mutations, as discussed at the beginning of the article, are benign and
are referred to merely as hemoglobin
variants.
There
is a group of genetic disorders, known as the porphyrias
that are characterized by errors in metabolic pathways of heme synthesis. King George
III of the United Kingdom was probably the most famous porphyria
sufferer.
To
a small extent, hemoglobin A slowly combines with glucose
at a certain location in the molecule. The resulting molecule is often referred
to as Hb
A1c. As the concentration
of glucose in the blood increases, the percentage of Hb A that turns into Hb A1c
increases. In diabetics
whose glucose usually runs high, the percent Hb A1c also runs high.
Because of the slow rate of Hb A combination with glucose, the Hb A1c
percentage is representative of glucose level in the blood averaged over a
longer time (the half-life of red blood cells, which is typically 50-55 days).
Hemoglobin
levels are amongst the most commonly performed blood
tests, usually as part of a full blood count or complete
blood count. Results are reported in g/L,
g/dL
or mol/L.
For conversion, 1 g/dL is 0.621 mmol/L. If the total hemoglobin concentration
in the blood falls below a set point, this is called anemia.
Normal values for hemoglobin levels are:
· Women:
12.1 to 15.1 g/dl
· Men:
13.8 to 17.2 g/dl
· Children:
11 to 16 g/dl
· Pregnant
women: 11 to 12 g/dl [5]
Anemias
are further subclassified by the size of the red blood cells, which are the
cells which contain hemoglobin in vertebrates. They can be classified as
microcytic (small sized red blood cells), normocytic (normal sized red blood
cells), or macrocytic (large sized red blood cells). The hemaglobin is the
typical test used for blood
donation. A comparison with the hematocrit
can be made by multiplying the hemaglobin by three. For example, if the
hemaglobin is measured at 17, that compares with a hematocrit of .51.[6]
Glucose
levels in blood can vary widely each hour, so one or only a few samples from a
patient analyzed for glucose may not be representative of glucose control in
the long run. For this reason a blood sample may be analyzed for Hb A1c
level, which is more representative of glucose control averaged over a longer
time period (determined by the half-life of the individual's red blood cells,
which is typically 50-55 days). People whose Hb A1c runs 6.0% or
less show good longer-term glucose control. Hb A1c values which are
more than 7.0% are elevated. This test is especially useful for diabetics.[8]
There
are several kinds of lymphocytes (although they all look alike under the
microscope), each with different functions to perform . The most common types of lymphocytes are
Although bone marrow is the ultimate
source of lymphocytes, the lymphocytes that will become T cells migrate from
the bone marrow to the thymus
where they mature. Both B cells and T cells also take up residence in
lymph nodes, the spleen and other tissues where they
Monocytes
leave the blood and become macrophages and dendritic cells.
This
scanning electron micrograph (courtesy of Drs. Jan M. Orenstein and Emma
Shelton) shows a single macrophage surrounded by several lymphocytes.
Macrophages
are large, phagocytic cells that engulf
Platelets
are cell fragments produced from megakaryocytes.
Blood
normally contains 150,000–350,000 per microliter (µl) or cubic millimeter (mm3).
This number is normally maintained by a homeostatic (negative-feedback)
mechanism .
If
this value should drop much below 50,000/µl, there is a danger of uncontrolled
bleeding because of the essential role that platelets have in blood clotting.
Some
causes:
When
blood vessels are cut or damaged, the loss of blood from the system must be
stopped before shock and possible
death occur. This is accomplished by solidification of the blood, a process
called coagulation or clotting.
A
blood clot consists of
Plasma is the straw-colored liquid in which the blood
cells are suspended.
Plasma
transports materials needed by cells and materials that must be removed from
cells:
Most
of these materials are in transit from a place where they are added to the
blood (a "source")
to
places ("sinks") where they will be removed from the blood.
Proteins
make up 6–8% of the blood. They are about equally divided between serum
albumin and a great variety of serum globulins.
After
blood is withdrawn from a vein and allowed to clot, the clot slowly shrinks. As
it does so, a clear fluid called serum is squeezed out. Thus:
Serum is blood plasma without fibrinogen and other
clotting factors.
The
serum proteins can be separated by electrophoresis.
·
A
drop of serum is applied in a band to a thin sheet of supporting material, like
paper, that has been soaked in a slightly-alkaline salt solution.
·
At
pH 8.6, which is commonly used, all the proteins are negatively charged, but
some more strongly than others.
·
A
direct current can flow through the paper because of the conductivity of the
buffer with which it is moistened.
·
As
the current flows, the serum proteins move toward the positive electrode.
·
The
stronger the negative charge on a protein, the faster it migrates.
·
After
a time (typically 20 min), the current is turned off and the proteins stained
to make them visible (most are otherwise colorless).
·
The
separated proteins appear as distinct bands.
·
The
most prominent of these and the one that moves closest to the positive
electrode is serum albumin.
·
Serum
albumin
o
is
made in the liver
o
binds
many small molecules for transport through the blood
o
helps
maintain the osmotic pressure
of the blood
·
The
other proteins are the various serum globulins.
·
They
migrate in the order
o
alpha
globulins (e.g., the proteins that transport thyroxine and retinol [vitamin A])
o
beta
globulins (e.g., the iron-transporting protein
transferrin)
o
gamma
globulins.
§
Gamma
globulins are the least negatively-charged serum proteins. (They are so weakly
charged, in fact, that some are swept in the flow of buffer back toward the
negative electrode.)
§
Most
antibodies are gamma globulins.
§
Therefore
gamma globulins become more abundant following infections or immunizations.
Albumins – multidispersed fraction of blood plasma
which are characterized by the high
electrophoretic mobility and mild dissolubility in water and saline solutions.
Molecular weight of albumins is about 60000. Due to high hydrophilic properties
albumins bind a significant amount of water, and the volume of their molecule
under hydratation is doubled. Hydrative layer formed around the serum albumins
provides to 70-80 % of oncotic pressure of blood plasma proteins, that can be
applied in clinical practice at albumins transfusion to patients with tissue
edemas. The decreasing of albumins concentration in blood plasma, for example
under disturbance of their synthesis in hepatocytes at liver failure, can cause
the water transition from a vessels into the tissues and development of oncotic
edemas.
Albumins
execute also important physiological function as transporters of a lot of
metabolites and diverse low molecular weight structures. The molecules of
albumins have several sites with centers
of linkage for molecules of organic ligands, which are affixed by the electrostatic
and hydrophobic bonds. Serum albumins can affix and convey fatty acids,
cholesterol, cholic pigments (bilirubin and that similar), vitamins, hormones,
some amino acids, toxins and medicines.
Albumins also
execute the buffer function. Due to the availability in their structure amino
and carboxylic groups albumins can react both as acids and as alkaline.
Albumins can
bound different toxins in blood plasma (bilirubin, foreign substances et c.).
This is the desintoxicative function of
albumins.
Albumins also
play role of amino acids depot in the organism. They can supply amino acids for
the building of another proteins, for example enzymes.
Globulins -
heterogeneous fraction of blood proteins which execute transport (a1-globulins –
transport of lipids, thyroxin, corticosteroid hormones; a2-globulins -
transport of lipids, copper ions; b-globulins -
transport of lipids, iron) and protective (participation of b-globulins in
immune reactions as antitoxins; g-globulins as
immunoglobulins) functions. They also support the blood oncotic pressure and
acid-alkaline balance, provide amino acids for the organism requirements. The
molecular weight of globulins is approximately 150000-300000.
The globulin
level in blood plasma is 20-40 g/l. A ratio between concentrations of albumins
and globulins (so called “protein coefficient”) in blood plasma is often
determined in clinical practice. In healthy people this coefficient is 1,5-2,0.
Fibrinogen – important protein of blood plasma, precursor of fibrin, the
structural element of blood clots. Fibrinogen participates in blood clotting
and thus prevents the loss of blood from the vascular system of vertebrates.
The approximate molecular weight of fibrinogen is 340000. It is the complex
protein, it contains the carbohydrate as prosthetic group. The content of
firinogen in blood is 3-4 g/l.
Subfractions of a1, a2, b and g globulins, their structure and
functions.
Immunoglobulins (Ig A, Ig G, Ig E, Ig M) - proteins of g-globulin
fraction of blood plasma executing the functions of antibodies which are the
main effectors of humoral immunity. They appear in the blood serum and certain
cells of a vertebrate in response to the introduction of a protein or some
other macromolecule foreign to that species.
Immunoglobulin
molecules have bindind sites that are specific for and complementary to the
structural features of the antigen that induced their formation. Antibodies are
highly specific for the foreign proteins that evoke their formation.
Molecules of
immunoglobulins are glycoproteins. The
protein part of immunoglobulins contain
four polipeptide chains: two heavy H-chains and two light L-chains.
C-reactive
protein (g-fraction).
This protein received the title owing to its capacity to react with
C-polysaccharide of a pneumococcus forming precipitates. According to its
chemical nature C-reactive protein is glycoprotein.
In blood
plasma of healthy people the C-reactive protein is absent but it occurs at
pathological states accompanied by an inflammation and necrosis of tissues. The
availability of C-reactive protein is characteristic for the acute period of
diseases – “protein of an acute phase”. The determination of C-reactive protein
has diagnostic value in an acute phase of rheumatic disease, at a myocardial
infarction, pneumococcal, streptococcal, staphylococcal infections.
Crioglobulin - the protein
of the g-globulin
fraction. Like to the C-reactive protein crioglobulin absent in blood plasma of
the healthy people and occurs at leukoses, rheumatic disease, liver cirrhosis,
nephroses. The characteristic physico-chemical feature of crioglobulin is its
dissolubility at standard body temperature (37 oC) and capacity to
form the sediment at cooling of a blood plasma up to 4 oC.
a2-macroglobulin - protein of a2-globulin
fraction, universal serum proteinase inhibitor. Its contents (2,5 g/l) in blood
plasma is highest comparing to another proteinase inhibitors.
The biological
role of a2-macroglobulin
consists in regulation of the tissue proteolysis systems which are very
important in such physiological and pathological processes as blood clotting,
fibrinolysis, processes of immunodefence, functionality of a complement system,
inflammation, regulation of vascular tone (kinine and renin-angiothensine
system).
a1-antitrypsin (a1-globulin) –
glycoprotein with a molecular weight 55 kDa. Its concentration in blood plasma
is 2-3 г/л. The main biological property of this inhibitor is its capacity to
form complexes with proteinases oppressing proteolitic activity of such enzymes
as trypsin, chemotrypsin, plasmin, trombin. The content of a1-antitrypsin
is markedly increased in inflammatory processes. The inhibitory activity of a1-antitrypsin
is very important in pancreas necrosis and acute pancreatitis because in these
conditions the proteinase level in blood and tissues is sharply increased. The
congenital deficiency of a1-antitrypsin
results in the lung emphysema.
Fibronectin –
glycoprotein of blood plasma that is synthesized and secreted in intercellular
space by different cells. Fibronectin present on a surface of cells, on the
basal membranes, in connective tissue and in blood. Fibronectin has properties
of a «sticking» protein and contacts with the carbohydrate groups of
gangliosides on a surface of plasma membranes executing the integrative
function in intercellular interplay. Fibronectin also plays important role in
the formation of the pericellular matrix.
Haptoglobin - protein of a2-globulin
fraction of blood plasma. Haptoglobin
has capacity to bind a free haemoglobin forming a complex that refer to b-globulins
electrophoretic fraction. Normal concentration in blood plasma - 0,10-0,35 g/l.
Haptoglobin-hemoglobin
complexes are absorbed by the cells of reticulo-endothelial system, in
particular in a liver, and oxidized to cholic pigments. Such haptoglobin
function promotes the preservation of iron ions in an organism under conditions
of a physiological and pathological erythrocytolysis.
Transferrin -
glycoprotein belonging to the b-globulin
fraction. It binds in a blood plasma iron ions (Fe3+). The protein
has on the surface two centers of linkage of iron. Transferrin is a transport
form of iron delivering its to places of
accumulation and usage.
Ceruloplasmin -
glycoprotein of the a2-globulin
fraction. It can bind the copper ions in blood plasma. Up to 3 % of all copper
contents in an organism and more than 90 % copper contents in plasma is
included in ceruloplasmin. Ceruloplasmin has properties of ferroxidase
oxidizing the iron ions. The decrease of
ceruloplasmin in organism (Wilson disease) results in exit of copper ions from
vessels and its accumulation in the connective tissue that shows by
pathological changes in a liver, main brain, cornea.
The place of synthesis of each
fraction and subfruction of blood plasma proteins.
Albumins, a1-globulins, fibrinogen are fully synthesized in
hepatocytes. Immunoglobulins are produced by plasmocytes (immune cells). In
liver cryoglobulins and some other g-globulins are produced too. a2-globulins and b-globulins are partly synthesized in
liver and partly in reticuloendothelial cells.
Causes and consequences of protein
content changes in blood plasma.
Hypoproteinemia - decrease of the total contents of proteins
in blood plasma. This state occurs in old people as well as in pathological
states accompanying with the oppressing of protein synthesis (liver diseases)
and activation of decomposition of tissue proteins (starvation, hard infectious
diseases, state after hard trauma and operations, cancer). Hypoproteinemia
(hypoalbuminemia) also occurs in kidney diseases, when the increased excretion
of proteins via the urine takes place.
Hyperproteinemia - increase of the total contents of proteins in
blood plasma. There are two types of
hyperproteinemia - absolute and relative.
Absolute hyperproteinemia – accumulation
of the proteins in blood. It occurs in infection and inflammatory diseases
(hyperproduction of immunoglobulins),
rheumatic diseases (hyperproduction of C-reactive protein), some
malignant tumors (myeloma) and others.
Relative hyperproteinemia – the increase of the protein concentration but
not the absolute amount of proteins. It occurs when organism loses water
(diarrhea, vomiting, fever, intensive physical activity etc.).
The principle of the measurement of
protein fractions by electrophoresis method.
Electrophoresis is the separation of
proteins on the basis of their electric charge. It depends ultimately on their
base-acid properties, which are largely determined by the number and types of
ionizable R groups in their polipeptide chains. Since proteins differ in amino
acid composition and sequence, each protein has distinctive acid-base
properties. There are a number of different forms of electroforesis useful for
analyzing and separating mixtures of proteins
If
a precursor of an antibody-secreting cell becomes cancerous, it divides
uncontrollably to generate a clone of plasma cells
secreting a single kind of antibody molecule. The image (courtesy of Beckman
Instruments, Inc.) shows — from left to right — the electrophoretic separation
of:
1.
normal human serum with its diffuse band of gamma
globulins;
2.
serum
from a patient with multiple myeloma producing an IgG myeloma protein;
3.
serum
from a patient with Waldenström's macroglobulinemia where the cancerous
clone secretes an IgM antibody;
4.
serum
with an IgA myeloma protein.
§
Gamma
globulins can be harvested from donated blood (usually pooled from several
thousand donors) and injected into persons exposed to certain diseases such as
chicken pox and hepatitis. Because such preparations of immune globulin
contain antibodies against most common infectious diseases, the patient gains
temporary protection against the disease.
Because
of their relationship to cardiovascular disease, the analysis of serum lipids
has become an important health measure.
The
table shows the range of typical values as well as the values above (or below)
which the subject may be at increased risk of developing atherosclerosis.
·
Total
cholesterol is the serum of blood
o
HDL
cholesterol
o
LDL
cholesterol and
o
20%
of the triglyceride value
·
Note
that
o
high
LDL values are bad, but
o
high
HDL values are good.
·
Using
the various values, one can calculate a
cardiac risk ratio = total cholesterol divided by HDL
cholesterol
A
cardiac risk ratio greater than 7 is considered a warning
What are the functions of the
liver?
http://www.youtube.com/watch?v=tat0QYxlCbo&feature=related
Liver’s functions:
• It is responsible
for the production of bile which is stored in the gallbladder and released when
required for the digestion of fats.
• The
liver stores glucose in the form of glycogen which is converted back to glucose
again when needed for energy.
• It
also plays an important role in the metabolism of protein and fats. It stores
the vitamins A, D, K, B12 and folate and synthesizes blood clotting factors.
•
Another important role is as a detoxifier, breaking down or transforming
substances like ammonia, metabolic waste, drugs, alcohol and chemicals, so that
they can be excreted. These may also be referred to as "xenobiotic"
chemicals. If we examine the liver under a microscope, we will see rows of
liver cells separated by spaces which act like a filter or sieve, through which
the blood stream flows. The liver filter is designed to remove toxic matter
such as dead cells, microorganisms, chemicals, drugs and particulate debris
from the blood stream. The liver filter is called the sinusoidal system, and
contains specialized cells known as Kupffer cells which ingest and breakdown
toxic matter.
http://www.youtube.com/watch?v=nXRWkorYFXc
Role of the liver in carbohydrate metabolism.
From intestine glucose pass into the
liver, where most part of it undergone the phosphorillation.
Glucose-6-phosphate formed in result of this reaction, which catalyzed by two
enzymes – hexokinase and glucokinase. When level of glucose in blood of v. porta
and in the hepatocytes is normal activity of glucokinase is low. After eating
activity of this enzyme increase and blood level of glucose decrease because
glucose-6-phosphate cannot pass through membrane.
http://www.youtube.com/watch?v=ejJRYozvuaw&feature=related
http://www.youtube.com/watch?v=nKgUBsC4Oyo&feature=related
Fructose and
galactose also transformed into glucose-6-phosphate in the liver.
Glucose-6-phosphate
is a key product of carbohydrates metabolism. In the liver this substance can
metabolized into different ways depend of liver’s and whole organism’s
necessity.
1. Synthesis
of glicogen. Content in the liver – 70-100g. After eating amount of glicogen in
the liver increase up to 150g. After 24 hours of starvation content of glicogen
in the liver decreases to zero and glukoneogenesis started.
2.
Glucose-6-phosphatase catalize dephosphorillation of glucose-6-phosphate and
free glucose formed. This enzyme is present in the liver, kidney and small
intestine. This process keep normal level of glucose in the blood.
3. Excess of
glucose-6-phosphate, which not used for synthesis of glicogen and forming of
free glucose, decomposites in glycolysis for pyruvate and for acetyl-CoA, which
are used for fatty acids synthesis.
4.
Glucose-6-phosphate decomposites for H2O and CO2, and free energy for
hepatocytes formed.
5. Part of glucose-6-phosphate
oxidized in pentosophosphate cycle. This way of glucose decomposition supplyes
reducted NADPH, which is necessary in fatty acid synthesis, cholesterin
synthesis, and also pentosophosphates for nucleic acids. Near 1/3 of glucose in
liver used for this pathway, another 2/3 – for glycolisis.
Hepatocytes
content full set of gluconeogenesis necessary enzymes. So, in liver glucose can
be formed from lactate, pyruvate, amino acids, glycerine. Gluconegenesis from
lactate takes place during intensive muscular work. Lactate formed from glucose
in muscles, transported to the liver, new glucose formed and transported to the
muscles (Kori cycle).
http://www.youtube.com/watch?v=qF3ylhC0VeQ
http://www.youtube.com/watch?v=CkwQJCtq6sE&feature=related
Role of the liver in lipid
metabolism.
In the liver
all processes of lipid metabolism take place. Most important of them are
following:
1. Lipogenesis (synthesis of
fatty acids and lipids). Substrate for this process – acetyl-CoA, formed from
glucose and amino acids, which are not used for another purposes. This process
is very active when the person eats a lot of carbohydrates. Liver more active than
another tissues synthesizes saturated and monounsaturated fatty acids. Fatty
acids then used for synthesis of lipids, phospholipids, cholesterol ethers.
Glycerol-3-phosphate, which is necessary for lipids synthesis, formed in liver
in result of two processes: from free glycerol under influence of
glycerolkinase, or in reducing of dioxiacetone phosphate under influence of
glycerolphosphate dehydrogenase. Active form of fatty acids interact with
glycerol-3-phosphate and phosphatidic acid formed, which used for synthesis of
triacylglycerines and glycerophospholipids.
http://www.youtube.com/watch?v=hRx_i9npTDU&feature=related
2. Liver play a central role
in synthesis of cholesterin, because near 80 % of its amount is synthesized
there. Biosynthesis of cholesterin regulated by negative feedback. When the
level of cholesterin in the meal increases, synthesis in liver decreases, and
back to front. Besides synthesis regulated by insulin and glucagon. Cholesterin
used in organism for building cell membranes, synthesis of steroid hormones and
vitamin D. Excess of cholesterin leads out in the bile to the intestine.
Another part of cholesterin used for bile acids synthesis. This process
regulated by reabsorbed bile acids according to negative feedback principles.
http://www.youtube.com/watch?v=hRx_i9npTDU&feature=related
3. Liver is a place of ketone
bodies synthesis. These substances formed from fatty acids after their
oxidation, and from liver transported to another tissues, first of all to the
heart, muscles, kidneys and brain. These substances are main source of energy
for many tissues of our organism excepting liver in normal conditions (heart)
and during starvation (brain).
http://www.youtube.com/watch?v=mLi9SEIrbuc&feature=related
Role of the liver in protein
metabolism.
Liver has
full set of enzymes, which are necessary for amino acids metabolism. Amino
acids from food used in the liver for following pathways:
1. Protein
synthesis.
2.
Decomposition for the final products.
3.
Transformation to the carbohydrates and lipids.
4.
Interaction between amino acids.
5.
Transformation to the different substances with amino group.
6. Release to
the blood and transport to another organs and tissues.
The high
speed of protein synthesis and decomposition is typical for the liver.
Hepatocytes catch different protein from blood (from hemolysated RBC,
denaturated plasma proteins, protein and peptide hormones) and decomposite them
to the free amino acids which used for new synthesis. When organism does not
get necessary quantity of amino acids from food, liver synthesizes only high
necessary proteins (enzymes, receptors).
Liver
syntesizes 100 % of albumines, 90 % of α1-globulines, 75 % of
α2-globulines, 50 % of β-globulines, blood clotting factors,
fibrinogen, protein part of blood lipoproteins, such enzyme as cholinesterase.
The speed of these processes is enough high, for example, liver synthesizes
12-16g of albumines per day.
Amino acids,
which are not used for protein synthesis, transformed to another substances.
Oxidative decomposition of amino acids is main source of energy for liver in
normal conditions.
Liver can
synthesize non-essential amino acids.
Liver
synthesizes purine and pyrimidine nucleotides, hem, creatin, nicotinic acid,
cholin, carnitin, polyamines.
The decomposition of
hemoglobin in tissues, bile pigments formation.
After a life
span of about 120 days the erythrocytes die. The dead erythrocytes are taken up
by the phagocytes of the reticuloendothelial system of the body. About 7 gram
of Hb is released daily from these phagocytosed erythrocytes. The Hb molecule
is broken down into 3 parts:
(i) The protein
(globin) part is utilized partly as such or along with other body proteins.
(ii) The iron
is stored in the reticuloendothelial cells and is reused for the synthesis of
Hb and other iron containing substances of the body.
(iii) The
porphyrin part is converted to bile pigment, i.e. bilirubin which is excreted
in bile.
The several stages, which are
involved in the formation of bile pigment from Hb and the farther fate of this
pigment, are given below:
1. Hemoglobin
dissociates into heme and globin.
2. Heme in
the presence of the enzyme, heme oxygenase, loses one molecule of CO and one atom
of iron in Fe3+ form producing biliverdin. In this reaction, the porphyrin ring
is cleaved by oxidation of the alpha methenyl bridge between pyrrole rings. The enzyme needs NADPH+H+
and O2.
Biliverdin
which is green in color is the first bile pigment to be produced; it is reduced
to the yellow-colored bilirubin, the main bile pigment, by the enzyme biliverdin reductase requiring
NADPH+H+.
Bilirubin is non-polar,
lipid soluble but water insoluble. Bilirubin is a very toxic compound. For
example, it is known to inhibit RNA and protein synthesis and carbohydrate
metabolism in brain. Mitochondria appear to be especially sensitive to its
effect. Bilirubin formed in reticuloendothelial cells then is associated
with plasma protein albumin to protect cells from the toxic effects. As this
bilirubin is in complex with plasma proteins, therefore it cannot pass into the
glomerular filtrate in the kidney; thus it does not appear in urine, even when
its level in the blood plasma is very high. However, being lipid soluble, it
readily gets deposited in lipid-rich tissues specially the brain.
This bilirubin
is called indirect
bilirubin or free
bilirubin or unconjugated bilirubin.
The
detoxication of indirect bilirubin takes place in the membranes of endoplasmatic reticulum
of hepatocytes. Here bilirubin interact with UDP-glucuronic acid and is
converted to the water soluble form -bilirubin mono- and diglucoronids. Another name
of bilirubin mono- and diglucoronids is conjugated bilirubin or direct
bilirubin or bound bilirubin. This reaction is catalized by UDP-glucoroniltransferase.
Conjugated
bilirubin is water soluble and is excreted by hepatocytes to the bile.
Conjugated (bound) bilirubin undergoes degradation in the intestine through the
action of intestinal microorganisms. Bilirubin is reduced and, mesobilirubin is formed.
Then mesobilirubin is reduced again and mesobilinogen is formed.
The reduction of mesobilinogen results in the formation of stercobilinogen (in a colon).
Stercobilinogen is oxidized and the chief pigment (brown color) of feces stercobilin is formed. A
part of mesobilinogen is reabsorbed by the mucous of intestine and via
the vessels of vena porta system enter liver. In hepatocytes mesobilinogen
is splitted to pyrol compounds which are excreted from the organism with bile. If
the liver has undergone degeneration mesobilinogen enter the blood and is
excreted by the kidneys. This mesobilinogen in urine is called urobilin, or true urobilin. Thus, true
urobilin can be detected in urine only in liver parenchyma disease.
Another bile
pigment that can be reabsorbed in intestine is stercobolinogen. Stercobolinogen
is partially reabsorbed in the lower part of colon into the haemorroidal
veins. From the blood stercobolinogen pass via the kidneys into the
urine where it is oxidized to stercobilin. Another name of urine stercobilin is false urobilin.
As mentioned
above, the conversion of bilirubin to mesobilirubin occurs under the influence
of intestinal bacteria. These bacteria are killed or modified when
broad-spectrum antibiotics are administered. The gut is sterile in the newborn
babies. Under these circumstances, bilirubin is not-converted to urobilinogen,
and the feces are colored yellow due to bilirubin. The feces may even become
green because some bilirubin is reconverted to green-colored biliverdin by
oxidation.
The total
bilirubin content in the blood serum is 1,7-20,5 micromol/l, indirect
(unconjugated) bilirubin content is 1,7-17,1 micromol/l and direct (conjugated)
bilirubin content is 0,86-4,3 micromol/l.
Differentiation between
unconjugated and conjugated bilirubin. Direct and indirect bilirubin.
Diazo reagent
which is a mixture of sulfanilic acid, HCI and NaN02 is added to the
serum. The conjugated bilirubin gives a reddish violet color with it and the maximum
color intensity is obtained within 30 seconds; this is called direct test.
The
unconjugated bilirubin does not give the direct test; however, it gives
indirect test in which alcohol or caffeine is also added which sets free the
bilirubin frum its complex with plasma proteins. Due to this difference in the
type of diazo reaction given by these two forms of bilirubin, the term direct
and indirect forms of bilirubin are also used to describe conjugated
and unconjugated forms of bilirubin.
Some other
differences between these two forms of bilirubin are given below:
The mechanism of jaundice development,
their biochemical characteristic.
Jaundice or
icterus
is the orange-yellow discoloration of body tissues which
is best seen in the skin and conjunctivae; it is caused by the presence of an
excess of bilirubin in the blood plasma and tissue fluids.
Depending upon the cause of an increased plasma bilirubin level, jaundice can
be classified as
(i) pre-hepatic,
(ii) hepatic and
(iii) post-hepatic
Pre-hepafic jaundice. This type of jaundice is due to a raised
plasma level of unconjugated bilirubin. It is due to an excessive breakdown of
red cells which leads to an increased production of uncongugated bilirubin; it
is also called haemolytic jaundice. As the liver is not able to excrete into the bile all
the bilirubin reaching it, the plasma bilirubin level rises and jaundice
results. This type of jaundice was in the past called acholuric jaundice
because the unconjugated bilirubin, being bound to plasma proteins, is not
excreted in the urine despite its high level in the plasma; the urine is also
without bile salts. Prehepatic jaundice is also seen in neonates (physiological
jaundice) especially in the premature ones because the enzyme UDP-glucuronyl
transferase is deficient. Moreover relatively more bilirubin is produced in-the
neonates because of excessive breakdown of red blood cells.
Hepatic jaundice.This is typically seen in viral
hepatitis. Several viruses are responsible for viral hepatitis and include
hepatitis A, B, C and D viruses. The liver cells are damaged: inflammation
produces obstruction of bile canaliculi due to swelling around them. This
cholestasis causes the bile to regurgitate into the blood through bile canaliculi.
The blood contains abnormally raised amount both of conjugated and unconjugated
bilirubin and bile salts which are excreted in the urine.
Post hepatic jaundice. This results when there is
extrahepatic cholestasis due to an obstruction in the biliary passages outside
the liver. In this way, the bile cannot reach the small intestine and therefore
the biliary passages outside as well as inside the liver are distended with
bile. This leads to damage to the liver and bile regurgitates into the blood.
The conjugated bilirubin and the bile salt levels of the blood are thus greatly
raised and both of these are excreted in the urine. Liver function tests will
vary according to the degree of obstruction, i.e complete or incomplete. If the
obstruction is complete, the stools become pale or clay-colored and the urine
does not have any stercobilin. The absorption of fat and fat soluble vitamins
also suffers due to a lack of bile salts. Excess of bile salts in the plasma
produces severe pruritus (itching).
Hemolytic
jaundice is characterized by
1.
Increase
mainly of unconjugated bilirubin in the blood serum.
2.
Increased
excretion of urobilinogen with urine.
3.
Dark brown
colour of feces due to high content of stercobilinogen.
Hepatic
jaundice is characterized by
1.Increased
levels of conjugated and unconjugated bilirubin in serum.
2.Dark
coloured urine due to the excessive excretion of bilirubin and urobilinogen.
3.Pale, clay
coloured stools due to the absence of
stercobilinogen.
4.Increased
activities of alanine and aspartate transaminases.
Obstructive
(post hepatic ) jaundice is characterized by
1.Increased
concentration mainly of conjugated bilirubin in serum.
2.Dark
coloured urine due to elevated excretion of bilirubin and clay coloured feces
due to absence of stercobilinogen.
Role of the liver in
detoxification processes.
A xenobiotics
is a compound that is foreign to the body. The principal classes of xenobiotics
of medical relevance are drugs, chemical cancerogens, and various compounds
that have found their way into our environment by one route or another
(insecticides, herbicides, pesticides, food additions, cosmetics, domestic
chemical substances). Most of these compounds are subject to metabolism
(chemical alteration) in the human body, with the liver being the main organ
involved; occasionally a xenobiotics may be excreted unchanged.
Some internal
substances also have toxic properties (for example, bilirubin, free ammonia,
bioactive amines, products of amino acids decay in the intestine). Moreover,
all hormones and mediatores must be inactivated.
Reactions of
detoxification take place in the liver. Big molecules like bilirubin excreted
with the bile to intestine and leaded out with feces. Small molecules go to the
blood and excreted via kidney with urine.
The metabolism of
xenobiotics has 2 phases:
In phase 1,
the major reaction involved is hydroxylation, catalyzed by members of a class
of enzymes referred to as monooxygenases or cytochrome P-450 species. These
enzymes can also catalyze deamination, dehalogenation, desulfuration,
epoxidation, peroxidation and reduction reaction. Hydrolysis reactions and
non-P-450-catalyzed reactions also occur in phase 2.
In phase 2,
the hydroxylated or other compounds produced in phase 1 are converted by
specific enzymes to various polar metabolites by conjugation with glucuronic
acid, sulfate, acetate, glutathione, or certain amino acids, or by methylation.
The overall purpose
of metabolism of xenobiotics is to increase their water solubility (polarity)
and thus facilitate their excretion from the body via kidney.Very hydrophobic
xenobiotics would persist in adipose tissue almost indefinitely if they were
not converted to more polar forms.
In certain
cases, phase 1 metabolic reaction convert xenobiotics from inactive to biologically
active compounds. In these instances, the original xenobiotics are referred to
as prodrugs or procarcinogens. In other cases, additional phase 1 reactions
convert the active compounds to less active or inactive forms prior to
conjugation. In yet other cases, it is the conjugation reactions themselves
that convert the active product of phase 1 to less active or inactive species,
which are subsequently excreted in the urine or bile. In a very few cases,
conjugation may actually increase the biologic activity of a xenobiotics.
Hydroxylation
is the chief reaction involved in phase 1. The responsible enzymes are called
monooxygenases or cytochrome P-450 species. The reaction catalyzed by a
monooxygenase is:
RH above can represent
a very widee variety of drugs, carcinogens, pollutants, and certain endogenous
compounds, such as steroids and a number of other lipids. Cytochrome P-450 is
considered the most versatile biocatalyst known. The importance of this enzyme
is due to the fact that approximately 50 % of the drugs that patients ingest
are metabolized by species of cytochrome P-450. The following are important
points concerning cytochrome P-450 species:
http://www.youtube.com/watch?v=3DgxjDalZW0
1. Like hemoglobin, they are
hemoproteins.
2. They are present in highest amount
in the membranes of the endoplasmic reticulum (ER) (microsomal fraction) of
liver, where they can make up approximately 20 % of the total protein. Thay are
also in other tissues. In the adrenal, they are found in mitochondria as well
as in the ER; the various hydroxylases present in that organ play an important role
in cholesterol and steroid biosynthesis.
3. There are at least 6 closely
related species of cytochrome P-450 present in liver ER, each with wide and
somewhat overlapping substrate specificities, that act on a wide variety of
drugs, carcinogens, and other xenobiotics in addition to endogenous compounds
such as certain steroids.
4. NADPH, not NADP, is involved in
the reaction mechanism of cytochrome P-450. The enzyme that uses NADPH to yield
the reduced cytochrome P-450 is called NADPH-cytochrome P-450 reductase.
5. Lipids are also components of the
cytochrome P-450 system. The preferred lipid is phosphatidylcholine, which is
the major lipid found in membranes of the ER.
6. Most species of cytochrome P-450
are inducible. For instance, the administration of phenobarbital or of many
other drugs causes a hypertrophy of the smooth ER and a 3- to 4-fold increase
in the amount of cytochrome P-450 within 4-5 days. Induction of this enzyme has
important clinical implications, since it is a biochemical mechanism of drug
interaction.
7. One species of cytochrome P-450
has its characteristic absorption peak not at 450 nm but at 448 nm. It is often
called cytochrome-448.This species appears
to be relatively specific for the metabolism of polycyclic aromatic
hydrocarbons (PAHs) and related molecules; for this reason it is called
aromatic hydrocarbon hydroxylase (AHH). This enzyme is important in the
metabolism of PAHs and in carcinogenesis produced by this agents.
8. Recent findings have shown that
individual species of cytochrome P-450 frequently exist in polymorphic forms,
some of which exhibit low catalytic activity. These observation are one
important explanation for the variations in drug responses noted among many
patients.
http://www.youtube.com/watch?v=3DgxjDalZW0
In phase 1 reactions, xenobiotics are
generally converted to more polar, hydroxylated derivates. In phase 2 reactions,
these derivates are conjugated with molecules such as glucuronic acid, sulfate,
or glutatione. This renders them even more water-soluble, and they are
eventually excreted in the urine or bile.
There are at least 5 types of phase 2 reactions:
1. Glucuronidation. UDP-glucuronic acid is the glucuronyl donor, and a variety of glucuronyl
transferases, present in both the ER and cytosol, are the catalysts. Molecules
such as bilirubin, thyroxin, 2-acetylaminofluorene (a carcinogen), aniline,
benzoic acid, meprobromate (a tranquilizer), phenol, crezol, indol and skatol,
and many steroids are excreted as glucuronides. The glucuronide may be attached
to oxygen, nitrogen, or sulfur groups of substrates. Glucuronidation is
probably the most frequent conjugation reaction.
Glucuronidation, the combining of glucuronic acid with toxins,
requires the enzyme UDP-glucuronyl transferase (UDPGT). Many of the commonly prescribed drugs are detoxified
through this pathway. It also helps to detoxify aspirin, menthol, vanillin
(synthetic vanilla), food additives such as benzoates, and some hormones.
Glucuronidation appears to work well, except for those with Gilbert's syndrome--a relatively common
syndrome characterized by a chronically elevated serum bilirubin level (1.2-3.0
mg/dl). Previously considered rare, this disorder is now known to affect as
much as 5% of the general population. The condition is usually without serious
symptoms, although some patients do complain about loss of appetite, malaise,
and fatigue (typical symptoms of impaired liver function). The main way this
condition is recognized is by a slight yellowish tinge to the skin and white of
the eye due to inadequate metabolism of bilirubin, a breakdown product of
hemoglobin. The activity of UDPGT is increased by foods rich in the monoterpene
limonene (citris peel, dill weed oil, and caraway oil). Methionine,
administered as SAM, has been shown to be quite beneficial in treating Gilbert's
syndrome.
2. Sulfation. Some alcohols, arylamines, and phenols are sulfated. The sulfate donor
in these and other biologic sulfation reactions is adenosine
3´-phosphate-5´-phosphosulfate (PAPS); this compound is called
active sulfate.
Sulfation is the conjugation of
toxins with sulfur-containing compounds. The sulfation system is important for
detoxifying several drugs, food additives, and, especially, toxins from
intestinal bacteria and the environment. In addition to environmental toxins,
sulfation is also used to detoxify some normal body chemicals and is the main
pathway for the elimination of steroid and thyroid hormones. Since sulfation is
also the primary route for the elimination of neurotransmitters, dysfunction in
this system may contribute to the development of some nervous system disorders.
Many factors influence the activity
of sulfate conjugation. For example, a diet low in methionine and cysteine has
been shown to reduce sulfation. Sulfation is also reduced by excessive levels
of molybdenum or vitamin B6 (over about 100 mg/day). In some cases,
sulfation can be increased by supplemental sulfate, extra amounts of
sulfur-containing foods in the diet, and the amino acids taurine and
glutathione.
Sulfoxidation is the process by which
the sulfur-containing molecules in drugs and foods are metabolized. It is also
the process by which the body eliminates the sulfite food additives used to
preserve many foods and drugs. Various sulfites are widely used in potato salad
(as a preservative), salad bars (to keep the vegetables looking fresh), dried
fruits (sulfites keep dried apricots orange), and some drugs. Normally, the
enzyme sulfite oxidase metabolizes sulfites to safer sulfates,
which are then excreted in the urine. Those with a poorly functioning
sulfoxidation system, however, have an increased ratio of sulfite to sulfate in
their urine. The strong odor in the urine after eating asparagus is an
interesting phenomenon because, while it is unheard of in China, 100% of the
French have been estimated to experience such an odor (about 50% of adults in
the U.S. notice this effect). This example is an excellent example of genetic
variability in liver detoxification function. Those with a poorly functioning
sulfoxidation detoxification pathway are more sensitive to sulfur-containing
drugs and foods containing sulfur or sulfite additives. This is especially
important for asthmatics, which can react to these additives with
life-threatening attacks. Molybdenum helps asthmatics with an elevated ratio of
sulfites to sulfates in their urine because sulfite oxidase is dependent upon
this trace mineral.
3. Conjugation with
Glutathione. Glutathione (γ-glutamylcysteinylglycine) is a
tripeptide consisting of glutamic acid, cysteine, and glycine. Glutathione is
commonly abbreviated to GSH; the SH indicates the sulfhydryl group of its
cysteine and is the business part of the molecule. A number of potentially
toxic electrophilic xenobiotics (such as certain carcinogens) are conjugated to
the nucleophilic GSH. The enzymes catalyzing these reactions are called
glutathione S-transferases and are present in high amounts in liver cytosol and
in lower amounts in other tissues. glutathione conjugates are subjected to
further metabolism before excretion. The glutamyl and glycinyl groups belonging
to glutathione are removed by specific enzymes, and an acetyl group (donated by
acetyl-CoA) is added to the amino group of the remaining cystenyl moiety. The
resulting compound is a mercapturic acid, a conjugate of L-acetylcysteine,
which is then excreted in the urine.
Glutathione is also an
important antioxidant. This combination of detoxification and free radical
protection, results in glutathione being one of the most important
anticarcinogens and antioxidants in our cells, which means that a deficiency is
cause of serious liver dysfunction and damage. Exposure to high levels of
toxins depletes glutathione faster than it can be produced or absorbed from the
diet. This results in increased susceptibility to toxin-induced diseases, such
as cancer, especially if phase I detoxification system is highly active.
Disease states due to glutathione deficiency are not uncommon.
A deficiency can be induced either by
diseases that increase the need for glutathione, deficiencies of the nutrients
needed for synthesis, or diseases that inhibit its formation. Smoking increases
the rate of utilization of glutathione, both in the detoxification of nicotine
and in the neutralization of free radicals produced by the toxins in the smoke.
Glutathione is available through two routes: diet and synthesis.
Dietary glutathione (found in fresh fruits and vegetables, cooked fish, and
meat) is absorbed well by the intestines and does not appear to be affected by
the digestive processes. Dietary glutathione in foods appears to be efficiently
absorbed into the blood. However, the same may not be true for glutathione
supplements.
In healthy individuals, a daily
dosage of 500 mg of vitamin C may be sufficient to elevate and maintain good
tissue glutathione levels. In one double-blind study, the average red blood
cell glutathione concentration rose nearly 50% with 500 mg/day of vitamin C.
Increasing the dosage to 2,000 mg only raised red blood cell (RBC) glutathione
levels by another 5%. Vitamin C raises glutathione by increasing its rate of
synthesis. In addition, to vitamin C, other compounds which can help increase
glutathione synthesis include N-acetylcysteine (NAC), glycine,
and methionine. In an effort to increase antioxidant status in
individuals with impaired glutathione synthesis, a variety of antioxidants have
been used. Of these agents, only microhydrin, vitamin C and NAC have
been able to offer some possible benefit.
Over the past 5-10 years, the use of
NAC and glutathione products as antioxidants has become increasingly popular
among nutritionally oriented physicians and the public. While supplementing the
diet with high doses of NAC may be beneficial in cases of extreme oxidative
stress (e.g. AIDS, cancer patients going through chemotherapy, or drug
overdose), it may be an unwise practice in healthy individuals.
4. Acetylation. These
reactions is represented by X +
Acetyl-CoA → Acetyl-X + CoA, where X represents a xenobiotic. These
reactions are catalyzed by acetyltransferases present in the cytosol of various
tissues, particularly liver. The different aromatic amines, aromatic amino
acids, such drug as isoniazid, used in the treatment of tuberculosis, and
sulfanylamides are subjects to acetylation. Polymorphic types of
acetyltransferases exist, resulting in individuals who are classified as slow
or fast acetylators, and influence the rate of clearance of drugs such as
isoniazid from blood. Slow acetylators are more subject to certain toxic effects
of isoniazid because the drug persists longer in these individuals.
Conjugation of toxins with acetyl-CoA
is the primary method by which the body eliminates sulfa drugs. This system
appears to be especially sensitive to genetic variation, with those having a
poor acetylation system being far more susceptible to sulfa drugs and other
antibiotics. While not much is known about how to directly improve the activity
of this system, it is known that acetylation is dependent on thiamine,
pantothenic acid, and vitamin C.
5. Methylation. A few
xenobiotics (amines, phenol, tio-substances, inorganic compounds of sulphur,
selen, mercury, arsenic) are subject to methylation by methyltransferases,
employing S-adenosylmethionine as methyl donor. Also catecholamines and
nicotinic acid amid (active form of vitamin PP) are inactivated due to
methylation.
Very important way of detoxification
is ureogenes (urea synthesis). Free ammonia, which formed due to metabolism of
amino acids, amides and amines, removed from organism in shape of urea.
Methylation involves conjugating methyl
groups to toxins. Most of the methyl groups used for detoxification come
from S-adenosylmethionine (SAM). SAM is synthesized from the amino acid
methionine, a process which requires the nutrients choline, vitamin B12,
and folic acid. SAM is able to inactivate estrogens (through methylation), supporting
the use of methionine in conditions of estrogen excess, such as PMS. Its
effects in preventing estrogen-induced cholestasis (stagnation of bile
in the gall bladder) have been demonstrated in pregnant women and those on oral
contraceptives. In addition to its role in promoting estrogen excretion,
methionine has been shown to increase the membrane fluidity that is typically
decreased by estrogens, thereby restoring several factors that promote bile
flow. Methionine also promotes the flow of lipids to and from the liver in
humans. Methionine is a major source of numerous sulfur-containing compounds,
including the amino acids cysteine and taurine.
Nutritional
factors
Antioxidant vitamins like vitamin C,
beta-carotene, and vitamin E are obviously quite important in protecting the
liver from damage as well as helping in the detoxification mechanisms, but even
simple nutrients like B-vitamins, calcium, and trace minerals are critical in
the elimination of heavy metals and other toxic compounds from the body. The
lipotropic agents, choline, betaine, methionine, vitamin B6, folic
acid, and vitamin B12, are useful as they promote the flow of fat
and bile to and from the liver. Lipotropic formulas have been used for a wide
variety of conditions by nutrition-oriented physicians including a number of
liver disorders such as hepatitis, cirrhosis, and chemical-induced liver
disease. Lipotropic formulas appear to increase the levels of SAM and
glutathione. Methionine, choline, and betaine have been shown to increase the
levels of SAM.
Botanical
medicines
There is a long list of plants which
exert beneficial effects on liver function. However, the most impressive
research has been done on silymarin, the flavonoids extracted from silybum
marianum (milk thistle). These compounds exert a substantial effect on
protecting the liver from damage as well as enhancing detoxification processes.
Silymarin prevents damage to the liver through several mechanisms: by acting as
an antioxidant, by increasing the synthesis of glutathione and by increasing
the rate of liver tissue regeneration. Silymarin is many times more potent in
antioxidant activity than vitamin E and vitamin C. The protective effect of
silymarin against liver damage has been demonstrated in numerous experimental
studies. Silymarin has been shown to protect the liver from the damage produced
by such liver-toxic chemicals as carbon tetrachloride, amanita toxin,
galactosamine, and praseodymium nitrate.
One of the key mechanisms by which
silymarin enhances detoxification is by preventing the depletion of
glutathione. Silymarin not only prevents the depletion of glutathione induced
by alcohol and other toxic chemicals, but has been shown to increase the level
of glutathione of the liver by up to 35%, even in normals. Inhuman studies,
silymarin has been shown to have positive effects in treating liver diseases of
various kinds, including cirrhosis, chronic hepatitis, fatty infiltration of
the liver, and inflammation of the bile duct. The standard dosage for silymarin
is 70-210 mg three times/day.
Several amino acids (glyucine,
taurine, glutamine, arginine, and ornithine) are used to combine
with and neutralize toxins. Of these, glycine is the most commonly utilized in phase
II amino acid detoxification. Patients suffering from hepatitis, alcoholic
liver disorders, carcinomas, chronic arthritis, hypothyroidism, toxemia of
pregnancy, and excessive chemical exposure are commonly found to have a poorly
functioning amino acid conjugation system. For example, using the benzoate
clearance test (a measure of the rate at which the body detoxifies benzoate
by conjugating it with glycine to form hippuric acid, which is excreted by the
kidneys), the rate of clearance in those with liver disease is 50% of that in
healthy adults.
Even in apparently normal adults, a
wide variation exists in the activity of the glycine conjugation pathway. This
is due no only to genetic variation, but also to the availability of glycine in
the liver. Glycine, and the other amino acids used for conjugation, become
deficient on a low-protein diet and when chronic exposure to toxins results in
depletion.
Dietary
Changes
Adding certain supplements to your diet can stimulate detoxification. Fiber,
vitamin C and other antioxidants, chlorophyll, and glutathione (as the amino
acid L-cysteine) will all help. Herbs such as garlic, red clover, echinacea, or
cayenne may also induce some detoxification. Saunas, sweats, and niacin therapy
have been used to cleanse the body.
Simply increasing liquids and decreasing
fats will shift the balance strongly toward improved elimination and less toxin
buildup. Changes might include increased consumption of filtered water, herb
teas, fruits, and vegetables, as well as reducing fats, especially fried food,
meat and milk products. In general, moving from an acid-generating diet to a
more alkaline one will aid the process of detoxification. Acid-forming foods,
such as meats, milk products, breads and baked goods, and especially the
refined sugar and carbohydrate products, will increase body acidity and lead to
more mucus production and congestion, whereas the more alkaline vegetarian
foods enhance cleansing and clarity in the body.
A deeper level of detoxification diet
is made up exclusively of fresh fruits and vegetables, either raw and cooked,
and whole grains, both cooked and sprouted. This diet keeps fiber and water
intake high and helps colon detoxification. Most people can handle this well
and make the shift from their regular diet with a few days transition. Some
people do well on a brown rice fast (a more macrobiotic plan), usually for a
week or two, eating three to four bowls of rice daily along with liquids such
as teas."
Role of liver in excretion.
Bile is an important vehicle for bile
acid and cholesterol excretion, but it also removes many drugs, toxins, bile
pigments, and various inorganic substances such as copper, zinc, and mercury.
Evaluating of liver’s
functions.
Different methods are used for
evaluating of liver’s functions. Base for some of them is role of liver in proetin
metabolism (e.g. thymol’s test), for another – role of liver in detoxification
(indican’s test) or in excretion (checking of bilirubin level in blood). In all
cases physician must make a conclusion about disorder of liver’s functions
after complex investigation, because, as mentioned above, all metabolic ways
are present in liver.
The
liver filter can remove a wide range of microorganisms such as bacteria, fungi,
viruses and parasites from the blood stream, which is highly desirable, as we
certainly do not want these dangerous things building up in the blood stream
and invading the deeper parts of the body. Infections with parasites often come
from the contaminated water supplies found in large cities, and indeed other
dangerous organisms may find their way into your gut and blood stream from
these sources. This can cause chronic infections and poor health, so it is
important to protect your liver from overload with these microorganisms. The
safest thing to do is boil your water for at least 5 minutes, or drink only
bottled water that has been filtered and sterilized. High loads of unhealthy
microorganisms can also come from eating foods that are prepared in conditions
of poor hygiene by persons who are carrying bacteria, viruses or parasites on
their skin. Foods, especially meats that are not fresh or are preserved, also
contain a higher bacterial load, which will overwork the liver filter if they
are eaten regularly.
Recently,
it has become very fashionable for people to detoxify their bodies by various
means, such as fasting or cleansing the bowels with fiber mixtures. Fasting can
by its extreme nature, only be a temporary method of cleansing the body of
waste products, and for many people causes an excessively rapid release of
toxins which can cause unpleasant, acute symptoms. The liver filter, like any
filter, needs to be cleansed regularly, and it is much easier and safer to do
it everyday. This is easily and pleasantly achieved by adopting a daily eating
pattern that maintains the liver filter in a healthy clean state. By following
the methods and guidelines on this site, you will be able to keep the liver
filter healthy and clean. Although it is important to keep the intestines
moving regularly and to sweep their walls with high fiber and living foods, it
is important to remember that the bowels are really a channel of elimination
and not a cleansing organ per se. In other words the bowels cannot cleanse,
filter or remove toxic wastes from the blood stream.
The liver is the most important organ
in detoxification, as it is the body's premier cleansing organ. All the blood
in the body passes through the liver, which removes toxins, impurities, and
debris from the bloodstream.
The liver stores fat-soluble
substances; these can include chemicals, which can be stored in the liver for
years. Using enzymes, the liver transforms these chemicals into water-soluble
substances that can be excreted though the kidneys or the gastrointestinal
tract.
Hormones are metabolized by the
liver. Estrogen produced by the body and from hormone replacement therapies is
broken down. If estrogen is not adequately processed, excess estrogen can
result in endometriosis; high blood pressure; PMS; and breast, uterine, and
vaginal cancer.
The liver also manufactures bile to
digest fats; chemically changes many foods into vitamins and enzymes; converts
carbohydrates and proteins into glucose for brain fuel and glycogen for
muscular energy; and stores nutrients to be secreted as needed by the body to
build and maintain cells.
If the liver cannot perform these
jobs well, you may exhibit a number of symptoms. These include gas;
constipation; a feeling of fullness; loss of appetite; nausea after fatty
meals; an oily taste in the mouth; revulsion to fatty foods; frequent headaches
not related to stress; weak ligaments, tendons, and muscles; skin problems; and
emotional excesses.
Briefly put, living. What you eat,
where you live, and what you do all can affect the liver's performance. If you
consume a lot of processed foods, the additives can eventually affect the
liver. If you live in an area that is highly polluted, exposure to chemicals in
the air and water affects the liver. All of this can hurt the liver's
performance.
An impaired liver does not process food
or detoxify substances as rapidly or as completely as a healthy liver. If the
liver is not producing enough bile, it cannot adequately digest fats. If the
liver is detoxifying more slowly than it should, it can result in more toxic
substances circulating in the body.
If toxins continue to accumulate, the
liver may not be able to work fast enough to clean the blood. It is like being
on a treadmill that is going a little too fast: try as you might, you cannot go
forward, but instead are swept back into greater toxicity. Instead of being
converted into something useful or being eliminated, toxins remain unchanged.
They are eventually stored in fatty body tissue and in the cells of the brain
and central nervous system. The stored toxins may be slowly released to
recirculate in the blood, contributing to many chronic illnesses.
A toxin is basically any substance
that creates irritating and/or harmful effects in the body; stressing and
undermining one's biochemical health and organ function. Toxins can come from
by products of normal cell metabolism or from the outside environment e.g.
pollution, drugs, pesticides, dyes, chemicals, microbes, heavy metals, tobacco
smoke and so on.
Toxicity occurs when we take in more
then we can utilize and eliminate. Toxic chemicals can be a real problem, since
after years of exposure to these substances the body’s ability to eliminate
them can slow down. They can get recirculated into the bloodstream or stored in
the liver, body fat or other parts of the body. These types of buildups and
problems throughout the body can contribute to the development of serious
illnesses. Many chemicals are so widespread that we are unaware of them. But
they have worked their way into our bodies faster than they can be eliminated,
and are causing allergies and addictions in record numbers. The body's built in
detoxification apparatus include the respiratory, gastrointestinal, urinary,
skin and lymphatic systems.
Symptoms of Toxicity
Cancer and cardiovascular disease are two of the main toxicity-related
diseases. Arthritis, allergies, obesity, and many skin problems are others. In
addition, a wide range of symptoms, such as headaches, fatigue, pains, coughs,
gastrointestinal problems and problems from immune weakness can all be related
to toxicity.
Common indications of toxicity
include frequent, unexplained headaches, back or joint pain, tight or stiff
neck, arthritis, chronic respiratory or sinus problems, asthma, abnormal body odor,
bad breath, coated tongue, food allergies, poor digestion, chronic constipation
with intestinal bloating or gas, brittle nails and hair, psoriasis, adult acne,
unexplained weight gain over 10 pounds, unusually poor memory, chronic
insomnia, anxiety, depression, irritability, chronic fatigue, and environmental
sensitivities, especially to odors.
Detoxification is the process of
clearing toxins from the body or neutralizing them. Energy balancing and
detoxification herbal baths prompt the body to eliminate toxins from specific
areas of the body. As these toxins are released from the areas where they
have been stored, they move into the blood, lymph and other body fluids out of
the body through the urinary, gastrointestinal, lymphatic and respiratory
systems and the skin. The period of detoxification can be a few days, a
few weeks or a months depending on the extent, location and type of the
toxins in the body. As a person is detoxifying they may experience
uncomfortable symptoms including depression, mood changes, nausea, diarrhea ,
foggy head, fatigue, lack of energy, bad breathe, foul urine odour, foul
perspiration odour, body odour, sores, rashes, acne, cold or flu like symptoms,
headaches or any other symptom. This period where symptoms may seem to
worsen is sometimes called a healing crisis, but is actually just the body's
reacting to the presence of the toxins in the bloodstream and the movement of
the toxins out of the body. .
"The liver is one of the most
important organs in the body when it comes to detoxifying or getting rid of foreign
substances or toxins. The liver plays a key role in most metabolic processes,
especially detoxification. The liver neutralizes a wide range of toxic
chemicals, both those produced internally and those coming from the
environment. The normal metabolic processes produce a wide range of chemicals
and hormones for which the liver has evolved efficient neutralizing mechanisms.
However, the level and type of internally produced toxins increases greatly
when metabolic processes go awry, typically as a result of nutritional
deficiencies. These non-end-product metabolites have become a significant
problem in this age of conventionally grown foods and poor diets.
Many of the toxic chemicals the liver
must detoxify come from the environment: the content of the bowels and the
food, water, and air. The polycyclic hydrocarbons (DDT, dioxin, 2,4,5-T,
2,3-D, PCB, and PCP), which are components of various herbicides and
pesticides, are an example of chemicals that are now found in virtually all fat
tissues measured. Even those eating unprocessed organic foods need an effective
detoxification system because all foods contain naturally occurring toxic
constituents.
The liver plays several roles in
detoxification: it filters the blood to remove large toxins, synthesizes and
secretes bile full of cholesterol and other fat-soluble toxins, and
enzymatically disassembles unwanted chemicals. This enzymatic process usually
occurs in two steps referred to as phase I and phase II. Phase I
either directly neutralizes a toxin, or modifies the toxic chemical to form
activated intermediates which are then neutralized by one of more of the
several phase II enzyme systems.
Proper functioning of the liver's
detoxification systems is especially important for the prevention of cancer. Up
to 90% of all cancers are thought to be due to the effects of environmental
carcinogens, such as those in cigarette smoke, food, water, and air, combined
with deficiencies of the nutrients the body needs for proper functioning of the
detoxification and immune systems. The level of exposure to environmental
carcinogens varies widely, as does the efficiency of the detoxification
enzymes, particularly phase II. High levels of exposure to carcinogens coupled
with slow detoxification enzymes significantly increases susceptibility to
cancer.
One of the liver's primary
functions is filtering the blood. Almost 2 quarts of blood pass through the
liver every minute for detoxification. Filtration of toxins is absolutely
critical as the blood from the intestines contains high levels of bacteria,
bacterial endotoxins, antigen-antibody complexes, and various other toxic
substances. When working properly, the liver clears 99% of the bacteria and
other toxins during the first pass. However, when the liver is damaged, such as
in alcoholics, the passage of toxins increases by over a factor of 10.
The liver's second detoxification
process involves the synthesis and secretion of bile. Each day the liver
manufactures approximately 1 quart of bile, which serves as a carrier in which
many toxic substances are dumped into the intestines. In the intestines, the
bile and its toxic load are absorbed by fiber and excreted. However, a diet low
in fiber results in inadequate binding and reabsorption of the toxins. This
problem is magnified when bacteria in the intestine modify these toxins to more
damaging forms.
What happens when excretion of bile is
inhibited?
When the excretion of bile is
inhibited (i.e. cholestasis), toxins stay in the liver longer.
Cholestasis has several causes, including obstruction of the bile ducts and
impairment of bile flow within the liver. The most common cause of obstruction
of the bile ducts is the presence of gallstones. Currently, it is
conservatively estimated that 20 million people in the U.S. have gallstones.
Nearly 20% of the female and 8% of the male population over the age of 40 are
found to have gallstones on biopsy and approximately 500,000 gall bladders are
removed because of stones each year in the U.S. The prevalence of gallstones in
this country has been linked to the high-fat, low-fiber diet consumed by the
majority of Americans.
Impairment of bile flow within the
liver can be caused by a variety of agents and conditions. These conditions are
often associated with alterations of liver function in laboratory tests (serum
bilirubin, alkaline phosphatase, SGOT, LDH, GGTP, etc.) signifying cellular
damage. However, relying on these tests alone to evaluate liver function is not
adequate, since, in the initial or subclinical stages of many problems with
liver function, laboratory values remain normal. Among the symptoms people with
enzymatic damage complain of are:
Fatigue; general malaise; digestive
disturbances; allergies and chemical sensitivities; premenstrual syndrome;
constipation
Perhaps the most common cause of
cholestasis and impaired liver function is alcohol ingestion. In some
especially sensitive individuals, as little as 1 ounce of alcohol can produce
damage to the liver, which results in fat being deposited within the liver. All
active alcoholics demonstrate fatty infiltration of the liver. Methionine,
taken as SAM, has been shown to be quite beneficial in treating two common
causes of stagnation of bile in the liver--estrogen excess (due to
either oral contraceptive use or pregnancy) and Gilbert's syndrome.
Oranges and tangerines (as well as
the seeds of caraway and dill) contain limonene, a phytochemical that has
been found to prevent and even treat cancer in animal models. Limonene's
protective effects are probably due to the fact that it is a strong inducer of
both phase I and phase II detoxification enzymes that neutralize carcinogens.
Curcumin,
the compound that gives turmeric its yellow color, is interesting because it inhibits
phase I while stimulating phase II. This effect can be very useful in
preventing certain types of cancer. Curcumin has been found to inhibit
carcinogens, such as benzopyrene (found in charcoal-broiled
meat), from inducing cancer in several animal models. It appears that the
curcumin exerts its anti-carcinogenic activity by lowering the activation of
carcinogens while increasing the detoxification of those that are activated.
Curcumin has also been shown to directly inhibit the growth of cancer cells.
As most of the cancer-inducing
chemicals in cigarette smoke are only carcinogenic during the period between
activation by phase I and final detoxification by phase II, curcumin in the
turmeric can help prevent the cancer-causing effects of tobacco. Those exposed
to smoke, aromatic hydrocarbons, and other environmental carcinogens
will probably benefit from the frequent use of curry or turmeric.
The activity of phase I detoxification
enzymes decreases in old age. Aging also decreases blood flow through the
liver, further aggravating the problem. Lack of the physical activity necessary
for good circulation, combined with the poor nutrition commonly seen in the
elderly, add up to a significant impairment of detoxification capacity, which
is typically found in aging individuals. This helps to explain why toxic
reactions to drugs are seen so commonly in the elderly.
|
|
Liver failure, or hepatic failure,
is severe deterioration of liver function resulting from extensive damage of liver
cells. The syndrome respresents a severe clinical condition and is associated
with high mortality; therefore, a great challenge to intensive care
management.
Causes
Hepatic failure, on one hand, may be caused by viral hepatitis (particularly
B/C), drugs and intoxications. In these cases, hepatic failure is diagnosed
in the absence of chronic liver disease (fulminant liver failure). On the
other hand, hepatic failure often occurs at the terminal stage of chronic
hepatic illness, e.g. liver cirrhosis (acute-on-chronic liver failure).
Symptoms
Signs and symptoms of hepatic failure often include jaundice, a yellow
discoloration of the skin and vitreous body (white area) due to abnormally
high levels of bilirubin in the bloodstream. In addition, hepatic
encephalopathy occurs as brain function deteriorates due to toxic substances
in the blood. It is characterized by changes in logical thinking; changes in
personality and behavior; drowsiness; confusion; disorientation; impaired
and/or loss of consciousness; coma. Hepatic failure is further associated
with complications such as hypoglycemia, cerebral edema, metabolic acidosis,
coagulopathy and renal failure.
Pathobiochemistry
Corresponding to the manifold liver functions, hepatic failure disrupts most
of the body's functions. Major organs and systems such as the kidneys, the
central nervous system, the cardiovascular system, and the clotting system
are severely affected. Various substances, which are normally detoxified by
the liver, accumulate in blood; subsequently, patients with hepatic failure
suffer from intoxication because the body fails to remove poisonous
substances from the blood. Patients with hepatic failure usually have high
concentrations of the following in their bloodstream: bilirubin, bile acids,
certain amino acids, phenolic substances, ammonia.
|
|
|
Kidney functions in organism:
a) excretion of final metabolic
products;
b) maintaining of acid-base balance;
c) water-salts balance regulation;
d) endocrine function.
http://www.youtube.com/watch?v=6x5pVoMb_vI&feature=related
Physical and chemical characteristics and
components of urine:
a) volume,
physical and chemical properties of urine;
b) inorganic
components of urine;
c) organic
components of urine.
Key words
and phrases:
Kidney – the couple
organ, which is responsible for excriting of final products of metabolism and
for homeostasis. They regulate water and mineral metabolism, acid-base balance,
excriting of nitrogenous slags, osmotic pressure. Also they regulate arterial
pressure and erhythropoesis.
http://www.youtube.com/watch?v=glu0dzK4dbU
Nephron – is the structural and functional unit of
kidney.
Urine – fluid with different organic and inorganic
compouds, which must be excreted (excess of water, final products of nitrogen
metabolism, xenobiotics, products of protein’s decay, hormones, vitamins and
their derivates). Most of them present in urine in a bigger amount than in
blood plasma. So, urine formation – is not passive process (filtration and
diffusion only).
In basis of urine formation lay 3
processes: filtration, reabsorbtion and secretion.
Glomerulal filtration. Water and low weight molecules go to the urine with help of following
powers: blood hydrostatic pressure in glomerulas (near 70 mm Hg), oncotic
pressure of blood plasma proteins (near 30 mm Hg) and hydrostatic pressure of
plasma ultrafiltrate in glomerulal capsule (near 20 mm Hg). In normal
conditions, as You see, effective filtration pressure is about 20 mm Hg.
Hydrostatic pressure depends from
correlation between opening of a. afference and a. efference.
Primary urine formed in result of
filtration (about 200 L per day). Between all blood plasma substances only
proteins don’t present in a primary urine. Most of these substances are
undergone to the following reabsorbtion. Only urea, uric acid, creatinin, and
other final products of different metabolic pathways aren’t undergone to the
reabsorbtion.
For evaluate of filtration used clearance (clearance for some substance
– it is a amount of blood plasma in ml, which is cleaned from this substance
after 1 minute passing through kidney).
Drugs which stimulate blood
circulation in kidney (theophyllin), also stimulate filtration. Inflammatory
processes of renal tissue (nephritis) reduce filtration, and azotaemia occurred
(accumulation of urea, uric acid, creatinin, and other metabolic final
products).
Reabsorbtion. Lenght of renal tubules is about 100 km. So, all important for our
organism are reabsorbed during passing these tubules. Epitelium of renal
tubules reabsorb per day 179 L of water, 1 kg of NaCl, 500 g of NaHCO3,
250 g of glucose, 100 g of free amino acids.
All substances can be divided into 3
group:
1. Actively reabsorbed substances.
2. Substances, which are reabsorbed
in a little amount.
3. Non-reabsorbed substances.
To the first
group belong Na+, Cl-, Mg2+, Ca2+,
H2O, glucose and other monosaccharides, amino acids, inorganic
phosphates, hydrocarbonates, low-weight proteins, etc.
Na+ reabsorbed by active transport to
the epitelium cell, then – into the extracellular matrix. Cl- and
HCO3- following Na+ according to the
electroneutrality principle, water – according to the osmotic gradient. From
extracellular matrix substances go to the blood vessels. Mg2+ and Ca2+
are reabsorbed with help of special transport ATPases. Glucose and amino acids
use the energy of Na+ gradient and special carriers. Proteins are
reabsorbed by endocytosis.
Urea and uric acid are little
reabsorbable substances.
Creatinin, mannitol, inulin and some
other substances are non-reabsorbable.
Henle’s loop play important role in the
reabsobtion process. Its descendent and ascendent parts create anti-stream
system, which has big capacity for urine concentration and dilution. Fluid
which passes from proximal part of renal tubule to the descendent part of
Henle’s loop, where concentration of osmotic active substances higher than in
kidney cortex. This concentration is due to activity of thick ascendent part of
Henle’s loop, which is non-penetrated for water and which cells transport Na+
and Cl- into the interstitium. Wall of descendent part is penetrated
for water and here water pass into the interstitium by osmotic gradient but
osmotic active substances stay in the tubule. Ascendent part continue to
reabsorb salt hypertonically, even in the absence of aldosteron, so that fluid
entering the distal tubule still has a much lower osmolality than does
interstitial fluid.
Some substances (K+,
ammonia and other) are secreted into
urine in the distal part of tubules. K+ is changed to Na+
by the activity of Na+-K+ATPase.
Urinary System
Summary of Stages of Urine Formation
http://www.youtube.com/watch?v=aQZaNXNroVY&feature=related
I).
Summary Stages of filtration
A). Glomerular
filtration: small molecules enter tubule formed elements are too
big
B). Tubular
reabsorption: Molecules are reabsorbed into the blood stream.
From
the nephron into the capillary network.
i.e. Glucose is
actively reabsorbed by being transported on carriers. If the carriers are
overwhelmed glucose appears in the urine indicating diabetes.
C). Tubular
secretion: Substances are actively added to the tubular fluid
from the capillaries to the tube
II).
Mechanisms of Urine Formation
A). Glomerular
filtration:
hydrostatic
pressure or fluid pressure gradient
osmosis
B). Tubular
reabsorption:
diffusion
facilitated
diffusion
osmosis
active transport
C). Tubular
secretion:
active
transport
III).
Glomerular Filtration
Passive and
nonselective
Driven
hydrostatic pressure form the glomerular capillaries and the glomerular
capsule.
A). Filtration
membrane
B). Net
Filtration Pressure
(pressure going
in) –(pressure pushing out)
Glomerular
Hydrostatic Pressure: Pressure pushing out of the
glomerular capillaries
Colloid Osmotic
Pressure: Pressure pushing into the glomerular capillaries
because of differences in protein concentrations
Capsular
Hydrostatic Pressure: Pressure pushing into the
glomerular capillaries from fluid already in Bowman's capsule.
Glomerular
Hydrostatic Pressure- (Colloid Osmotic Pressure +Capsular Hydrostatic Pressure)
(force favoring
filtration)-(force opposing filtration)
C). Glomerular
Filtration Rate (GFR)
http://www.youtube.com/watch?v=lH9IXpp5zTU
1). surface area
2). permeability
3). Net Filtration Pressure
D). Control of glomerular
filtration
1). Intrinsic Controls:
Control from the renal system
regulating the diameter of
the afferent arteriole.
i). Myogenic Mechanism
ii). Tubuloglomerular feedback
mechanism
The osmoreceptors in distal
tubules respond to slowing flowing filtrate (thus decreased filtrate
concentration) by releasing vasodilators to the afferent
arterioles.
In response to fast filtrate rate
and thus high solute concentration by releasing vasoconstrictors.
Large diameter →
Increase volume→
Results in a high
net pressure →
And a fast GFR
(rate) →
so
there is no time to reabsorb →
Results in a high solute concentration
& high osmotic pressure at the
juxtaglomerular apparatus →
so
vasoconstrictor
will be released
Small diameter →
lowers volume →
Results in a low
net pressure →
And a slow GFR
(rate) →
so
there is too much time to reabsorb →
Results in a low solute concentration →
& low osmotic
pressure at the juxtaglomerular apparatus →
so
vasodilator will
be released
iii). Renin-Angiotensin mechanism
Osmoreceptors
release renin,
Renin acts on angiotensinogen,
angiotensin I
angiotensin II
angiotensin II is
a vasoconstrictor
blood pressure in the entire body to
rise
release aldosterone
aldosterone increases
reabsorption Na+
blood pressure increases
2). Extrinsic controls
(outside the renal system)
Sympathetic nerve fibers
the adrenal medulla
epinephrine
vasoconstriction in the afferent
arterioles
inhibits filtrate formation.
IV). Tubular Reabsorption
Concentrating of the filtrate by
returning solutes and water to the blood stream.
A). Methods of Reabsorption
1). Active Tubular Reabsorption
i). Cotransport
binding to the same as carrier
complex
That creates a transport maximum (Tm
mg/minute) for every solute.
When the carriers are exceeded the
solute is excreted in the urine.
( the Tm of glucose 375 mg/min
glucose over this limit is excreted).
ii). Pinocytosis
2). Passive Tubular Reabsorption
http://www.youtube.com/watch?v=aQZaNXNroVY&feature=related
i). tubular fluid
through the epithelium, into the interstitial fluid
then diffuse into the peritubular capillaries and back into the
blood
stream.
ii). Substances move
across their electrochemical gradient
iii). Positively
charged Na+ ions are actively transported
a). electrochemical
gradient
b). osmotic
gradient
B). Reabsorption
in different sections of the tubule.
http://www.youtube.com/watch?v=KINOArtDeWg&feature=related
1). Glomerular
capsule:
2). Proximal Convoluted
Tubule.
3). Loop of
Henle
Permeability
Water can leave descending
limb but not the ascending limb of the loop of Henle
Na+ cannot leave descending
limb but can leave the ascending limb of the loop of Henle
Countercurrent
Mechanism
Maintains the high
level of Na+ in the interstitial fluid
Fluid moving down
the descending limb creates a current that is counter to the fluid moving up
the ascending limb
Every time Na+ is
actively removed from the ascending limb;
water in the
descending limb is pulled out because of osmosis
So more Na+ that
is actively removed the more water is pulled out.
Mechanisms
Step a: Osmotic Gradient
Step b: Permeability to Solutes
The interstitial
fluid becomes hypertonic, but the filtrate becomes hypotonic.
(filtrate loses
salt it becomes increasingly dilute)
The loop creates a
concentration gradient along it length.
(countercurrent
multiplier.)
This gradient is what
causes the water to move out of the filtrate in the descending loop
Step c. Function of the Vasa Rectus
Step d Collecting Duct
Concentration of
fluid:
4). Distal
Convoluted Tubule
Water reabsorption
here is dependent on hormones.
5). Collecting Duct
V). Tubular
Secretion
Reabsorption in
reverse.
H+
K+
creatinine
ammonium ions
various drugs
VI). Hormones
affecting renal function
A). ADH:
B). Aldosterone:
C). Atrial
Natriuretic Peptide
Peculiarities of
biochemical processes in kidney.
Kidney have a
very high level of metabolic processes. They use about 10 % of all O2,
which used in organism. During 24 hours through kidney pass 700-900 L of blood.
The main fuel for kidney are carbohydrates. Glycolysis, ketolysis, aerobic
oxidation and phophorillation are very intensive in kidney. A lot of ATP formed
in result.
Metabolism of
proteins also present in kidney in high level. Especially, glutamine deaminase
is very active and a lot of free ammonia formed. In kidney take place the first
reaction of creatin synthesis.
Kidney have plenty
of different enzymes: LDG (1, 2, 3, 5), AsAT, AlAT. Specific for kidney is
alanine amino peptidase, 3rd isoform.
Utilization
of glucose in cortex and medulla is differ one from another. Dominative type of
glycolysis in cortex is aerobic way and CO2 formed in result. In
medulla dominative type is anaerobic and glucose converted to lactate.
Two sources
contribute to the renal ammonia: blood ammonia (is about one-third of excreted
ammonia), and ammonia formed in the kidney. The predominant source for ammonia
production within the kidney is glutamine, the most abundant amino acid in
plasma, but a small amount may originate
from the metabolism of other amino acids such as asparagine, alanine, and
histidine. Ammonia is secreted into the tubular lumen throughout the entire
length of the nephron. Secretion occurs both during normal acid-base balance
and in chronic acidosis.Metabolic acidosis is accompanied by an adaptive
increase in renal ammonia production with a corresponding increase in urinary
ammonium excretion.
Kidney cortex
like liver appear to be unique in that it possess the enzymatic potential for
both glucose synthesis from noncarbohydrate precursors (gluconeogenesis) and
glucose degradation via the glycolytic pathway. Gluconeogenesis is important
when the dietary supply of glucose does not satisfy the metabolic demands.
Under these conditions, glucose is required by the central nervous system, the
red blood cells, and possibly other tissues which cannot obtain all their energy
requirements from fatty acids or ketone body oxidation. Also, gluconeogenesis
may be important in the removal of excessive quantities of glucose precursors
from the blood (lactate acid after severe exercise for example). Although the
biosynthetic pathways are similar, there are several important differences in
the factors which regulate gluconeogenesis in the two organs. 1) The liver
utilizes predominately pyruvate, lactate and alanine. The kidney cortex
utilizes pyruvate, lactate, citrate, α-ketoglutarate,
glycine and glutamine. 2) Hydrogen ion activity has little effect upon
hepatic gluconeogenesis, but it has marked effects upon renal gluconeogenesis.
Thus, when intracellular fluid pH is reduced (metabolic acidosis, respiratory
acidosis or potassium depletion), the rates of gluconeogenesis in slices of
renal cortex are markedly increased. The ability of the kidney to convert
certain organic acids to glucose, a neutral substance, is an example of a
nonexcretory mechanism in the kidney for pH regulation.
Regulation of urine formation.
Na-uretic hormone
(produced in heart) decrease reabsorbtion of Na+, and quantity of
urine increased.
Aldosteron and some
other hormones (vasopressin, renin, angiotensin II) increase Na-reabsorbtion and decrease quantity of urine.
Role of kidney in acid-base
balance regulation.
Kidney have
some mechanisms for maintaining acid-base balance. Na+ reabsorbtion
and H+ secretion play very important role.
1. Primary
urine has a lot of Na2HPO4 (in dissociated form). When Na+
reabsorbed, H+ secreted into urine and NaH2PO4
formed.
2. Formation
of hydrocarbonates. Inside renal cells carboanhydrase forms from CO2
and H2O H2CO3, which dissociated to H+
and HCO3-. H+ excreted from cell into urine (antiport
with Na+) and leaded with urine. Na+ connect with HCO3-,
NaHCO3 formed and go to the blood, thereupon acidity decreased.
3. Formation
of free ammonia. NH3 used for formation of NH4+
(H+ ion associted), and different acid metabolites excreted as
ammonia salts.
Role of kidney in water
balance regulation.
Excessive entrance of water leads to dilution of
extracellular fluid. Decreasing of osmolality inhibits secretion of
antidiuretic hormone. Walls of collective tubules stay non-penetrated to water
and dilutive urine formed.
If volume of
blood circulation increases, circulation in kidney increases also and
hyperosmotic medium of kidney medulla removed. Some substances in these
conditions return into blood. So, excess of water carried with urine and a lot
of soluble substances are reabsorbed into blood. After water loading stopped,
hyperosmolality in kidney medulla returns for previous stage during some days.
Physical and chemical
characteristics of urine.
Urine amount
(diures) in healthy people is 1000-2000 ml per day. Day-time diures is in 3-4
times more than night-time.
Normal colour
of urine is yellow (like hay or amber), what is due to presence of urochrom
(derivate of urobilin or urobilinogen). Some another colour substances are
uroerythrin (derivate of melanine), uroporphyrines, rybophlavine and other.
Colour depends from urine concentration.
Urine is
transparent. This characteristic depends from amount of different salts
(oxalates, urates, phosphates), amount of present epitelium cells and
leucocytes.
Density of
urine depends from concentration of soluble substances. Borders of variation
are from 1002 to 1035 g/l. Near 60-65 g of hard substances are excreted with
urine per day.
In normal
conditions urine has acid or weak acid reaction (pH=5,3-6,8). This depends from
presence of NaH2PO4 and KH2PO4.
Fresh urine
has a specific smell, which is due to presence of flying acids. But a lot of microorganisms,
which are present in urine, split urea and free ammonia formed.
Organic compounds of urine.
Proteins. Healthy people excretes 30 mg of proteins per day. As a rule these are
low weight proteins.
Urea. This is main part of organic compounds in urine. Urea nitrogen is about
80-90 % of all urine nitrogen. 20-35 g of urea is excreted per day in
normal conditions.
Uric acid. Approximately 0,6-1,0 g of uric acid is excreted per day in form of
different salts (urates), mainly in form of sodium salt. Its amount depends
from food.
Creatinin and creatin. Near 1-2 g of creatinin is excreted per day, what depended from
weight of muscles. This is the constant for each person. Men excrete 18-32 mg
of creatinin per 1 kg of body weight per day, women – 10-25 mg. Creatinin
is non-reabsorbable substance, so this test used for evaluating of renal
filtration.
Amino acids. Per day healthy person excretes 2-3 g of amino acids (free amino acids
and different low weight molecule peptides). Also products of amino acids
metabolism can be found in the urine.
Couple substances. Hypuric acid (benzoyl glycine) is excreted in amount 0,6-1,5 g per day.
This index increases after eating a lot of berries and fruits, and in case of
protein’s decay in the intestines.
Indican (potassium salt of
indoxylsulfuric acid). Per day excrition of indican is
about 10-25 g. Increasing of indican’s level in urine is due to
inrtensification of decay proteins in the intestines and chronic diseases,
which are accompanied by intensive decopmosition of proteins (tuberculosis, for
example).
Organic acids. Formic, acetic, butyric, β-oxybutyric, acetoacetic and some other
organic acids are present in urine in a little amount.
Vitamines. Almost all vitamines can be excreted via kidney, especially,
water-soluble. Approximately 20-30 mg of vit C, 0.1-0.3 mg of vit B1,
0.5-0.8 mg of vit B2 and some products of vitamine’s metabolism.
These data can be used for evaluating of supplying our organism by vitamines.
Hormones. Hormones and their derivates are always present in urine. Their amount
depends from functional state of endocrinal glands and liver. There is a very
wide used test – determination of 17-ketosteroids in urine. For healthy man
this index is 15-25 g per day.
Urobilin. Present in a little amount, gives to urine yellow colour.
Bilirubin. In normal conditions present in so little amount that cannot be found by
routine methods of investigations.
Glucose. In normal conditions present in so little amount that cannot be found by
routine methods of investigations.
Galactose. Present in the newborn’s urine, when digestion of milk or transformation
of glalactose into glucose in the liver are violated.
Fructose. It is present in urine very seldom, after eating a lot of fruits,
berries and honey. In all other cases it indicates about liver’s
disorders, diabetes mellitus.
Pentoses. Pentoses are excreted after eating a lot of fruits, fruit juices, in
case of diabetes mellitus and steroid diabetes, some intoxications.
Ketone bodies. In normal conditions urine contains 20-50 mg of ketone bodies and this
amount cannot be found by routine methods of clinical investigations.
Porphyrines. Urine of healthy people contains a few I type porphyrines (up to 300 mkg
per day).
Inorganic compounds of urine.
Urine of
healthy people contains 15-25 g of inorganic compounds.
NaCl. Per day near 8-16 g of NaCl excreted with urine. This amount depends
from amount of NaCl in food.
Potassium. Twenty-four hours urine contains 2-5 g of K, which depends of amount of
plants in the food.
Different
drugs can change excretion of Na and K. For example, salicylates and
cortikosteroids keep Na and amplify excretion of K.
Calcium. Twenty-four hours urine contains 0.1-0.3 g, which depends from content
of calcium in the blood.
Magnesium. Content of magnesium in urine is 0.03-0.18 g. So little amount of
calcium and magnesium in urine can be explained by bad water solubility of
their salts.
Iron. Amount of iron in urine is about 1 mg per day.
Phosphorus. In urine are present one-substituted phosphates of potassium and sodium.
Their amount depends from blood pH. In case of acidosis two-substituted
phosphates (Na2HPO4) react with H+ and
one-substituted phosphates (NaH2PO4) formed. In case of
alkalosis one-substituted phosphates react with bases and two-substituted
phosphates formed. So, in both cases amount of phosphates in urine increases.
Sulfur. Amount of sulfur in twenty-four hours urine is 2-3 g per day (in form of
SO42-).
Ammonia. Ammonia is excreted in ammonium sulfates and couple substances. Ammonium
salts make up 3-6 % of all nitrogen in urine. Their amount depends from
character of food and blood pH.
Donald W. Seldin
Department of
Internal Medicine, The University of Texas Southwestern Medical School, Dallas,
Texas - USA
ABSTRACT: The
clearance concept is central to three critical areas of nephrology; it was a key
feature to early conceptual analysis of the nature of urine formation, it was
utilized as a measure of kidney function in advancing renal diseases, and it
was a pivotal concept to elucidate the physiology of the kidneys. This paper
describes the clearance concept as currently understood and then it examines
how clearance was utilized to understand these various aspects of kidney
function.
Key words:
Clearance concept, Johannes Muller, Carl Ludwig, Hans Driesch
The concept of
clearance is central to three major areas of nephrology. First, the nature of
urine for mation was explored to a great extent using clearance techniques.
Second, the early search for measures of kidney function with advancing disease
resorted to clearance procedures, particularly involving urea and creatinine.
Third, the physiology of the kidney was examined and developed with great power
and sophistication by the deepening theoretical understanding of the concept of
clearance accompanied by ingenious analytical techniques and procedures. There
is an additional domain which hovered over the studies of urine formation. This
had to do with the per vasive resort to vitalism as an explanation of
physiologic regulation. My task was to examine the birth and evolution of the
clearance concept. For purposes of exposition, it may be helpful to describe
first the clearance concept as it is currently understood and then recount how
the concept emerged and developed during the 19th and early 20th centuries, as
it was repeatedly invoked to analyze the process of urine formation, the
failure of renal function, and the nature of physiologic regulation.
Figure 1 gives the
definition of clearance in currently conventional units of time and
concentration. It is evident from the formula that the numerator is a rate of
excretion (mg/mm); the denominator is a plasma concentration (mg/mL).
Therefore, the clearance of any substance is expressed as mL/min (mg/min x
mL/mg=mL/min). Clearance, therefore, has the dimensions of a volume per unit
time. This simultaneous measurement of the excretion rate of a solute and a
flow rate of fluid from which the solute is derived has resulted in some
confusion. Fig 2, modified from Cassin and Vogh, emphasizes that the kidney
removes (clears) a small fraction of a substance from each mL of total flow.
The clearance, therefore, of any substance is the virtual volume of plasma flow
required to supply the amount of the substance excreted in any one minute.
The historical
evolution of the clearance concept is intimately connected with studies
examining the nature of urine formation. Particularly noteworthy reviews have
been published by Smith (2), Bradley (3), Thurau, Davis and Haberle (4),
Gottschalk (5), Schuster and Seldin (14). In the early 19th centur y, Johannes
Muller (18011858) advanced a theor y of urine formation that rested on two
prevalent concepts current at the time: 1) fluid movement was a secretory
process mediated by glands; 2) the activity of the secretor y system required
vitalistic forces that could not be reduced to physical processes. Despite
enormous contributions to microscopic anatomy, he denied that the glomerulus
was directly connected with the renal tubules, and ascribed urine formation to
the secretory activity of the tubules, regarding the kidney as a gland.
Notwithstanding the powerful currents of vitalism at the time, Carl Ludwig
(1816-1895) came to the study of kidney function with an uncompromising
physicochemical orientation. He appreciated the role of the afferent and
efferent arteriole in elevating the hydrostatic pressure in the intervening
glomerulus, thereby facilitating the movement of a protein-free ultrafiltrate,
containing all the elements to be found in the urine, and restraining the
passage of protein and formed elements. To account for the different
composition of blood and urine, Ludwig proposed that some unspecified chemical
force promoted active sodium chloride reabsorption while some property of the
tubular wall restrained urea back-diffusion. No vital force was postulated,
although the nature of the “chemical force” promoting reabsorption was
unspecified. Simultaneously and independently, William Bowman (1816-1892) also
postulated that water was separated from blood at the glomerulus, but he
assumed that solutes remained in the blood and were subsequently secreted into
the urine by the tubules. This was an expression of the prevalent view of
glandular secretion mediating solute movement. The central feature of Ludwig’s
theory that urine formation was critically linked with glomerular pressure, was
challenged by Rudolph Heidenhain (1834-1897). On the basis of calculations of a
clearance type, he concluded that to attribute urea excretion to filtration
alone would require 70 liters of filtrate and 68 liters of water reabsorption
per day. Heidenhain concluded that such circumstances were inconceivable, that
urine formation was linked with renal blood flow, not filtration pressure, and
that urine was derived from secretion by both glomerulus and tubules. When
Cushny (1866-1926) introduced his “modern view” in his monograph of 1917, he
accepted Ludwig’s thesis that the ultimate source of urine was filtration at
the glomerulus of non-colloid constituents by a purely physical process. He
rejected Heidenhain’s calculation as involving far too low an estimate of renal
blood flow; in addition, when the immense number of renal tubules are taken
into account, the requirement for water reabsorption could be reasonably accounted
for. Cushny rejected entirely the notion of tubular secretion. To account for
reabsorption, Cushny postu1ated some “vital activity” on the part of the
epilthelium – a postulate that Ludwig had steadfastly rejected. Thurau and his
associates (4) have pointed out that these various theories of urine formation
were unifed in a perceptive analysis by Metzner (1858-1935) published in 1906,
some ten years before Cushny’s “modern theory”.
Fig. 1
His conception of a
trifold process of ultrafiltration at the glomerulus by physical forces,
reabsorption of most of the filtrate in part by active tubular processes, and
active secretion of certain solutes by the tubular epithelia is remarkably
close to modern views. His summary is worth quoting (Fig. 3). It should be
emphasized that the use of clearance calculations by Heidenhain and their
reinterpretation by Cushny served to make creditable the conceptual model of
the comparatively modest magnitude of urine flow in a setting of huge volumes
of glomerular filtration.
Although Cushny
may have over-emphasized the commitment of Heidenhain and others to vitalism,
there is no question that the concept of vital activity, not reducible to
physical forces, was a powerful conceptual factor that infected the theories of
renal function. For most of the 19th centur y, a basic problem in biology was
conceived to be the distinction between living and non-living matter. A
mechanistic explanation assumed that organic and non-organic matter were not
irreducibly different. A vitalistic explanation assumed that a reduction of
living to non-living phenomena is in principle impossible. Embryology was a
dominating biologic discipline. To provide a flavor of the intellectual climate
surrounding the study of renal function, it may be helpful to review briefly
the prevailing embryologic studies. Landmark studies exemplified by the work of
Hans Driesch are summarized in a comprehensive publication in 1914 (7). In a
series of studies on embr yonic sea-urchins, he demonstrated that rearrangement
of cells at the blastomere stage had no effect on normal development. Moreover,
a single blastomere, isolated from the rest at the two - or fourcell stage, can
develop into a normal sea-urchin embr yo.
Fig. 2
The conclusion was
drawn that spatio temporal location is irrelevant to development, and that non-physical
forces “entelechies” are “wholemaking” factors which have no quantitative
characteristics. It was only the gradual advancement of physical and biologic
science that could meet the vitalistic arguments. Organic chemistr y was shown
to be a misnomer. The synthesis of urea, heretofore found only in living
organisms, from CO2 and NHby3 Wöhler in 1828 (7) led to the
view that organic chemistr y was simply the chemistr y of carbon compounds.
Purpose and purposiveness were explained by reference to integrated and
adjustible feed-back systems. The ability of blastomere cells to develop
differently in different transplant locations in ontogenesis, unlike a machine
where each part fulfills a designed function, is explainable in principle by
genetic theory. And finally “energy” input required to impart selectivity is
not confined to hydrostatic or oncotic forces. On a conceptual level, it was
pointed out by the logical positivist philosopher C.I. Hengel that vitalism has
no predictive power, offering neither verifiable predictions nor providing
models of coherent mechanisms. It was the increasing power of the physical
sciences that gradually undermined the recourse to postulated entities which
could not be identified, characterized, or worst of all, refuted. It was these
reasons which led Ludwig and Cushny to vigorously reject vitalistic
explanations.
Bright in 1836
recognized that the concentration of blood urea rose in patients with chronic
renal disease (3). Ambard (8) showed that the blood level of urea was related
to urea excretion and formulated an equation which was designed to register
impairment of renal function.
Fig. 3
However, the
equation involved a square root function which obscured the physiologic
significance of the relationship between urinar y excretion and blood urea
concentration. Addis (9), in 1917, showed that at maximal urine flows the ratio
of the excretion of urea per hour and the blood urea concentration was constant
in any one individual. This expression represented the urea clearance per hour,
an approximation of glomerular filtration rate. Austin, Stillman and Van Slyke
(10) showed that the rate of urine flow influenced urea excretion independently
of the blood level and renal excretory capacity. In a later study (11), it was
demonstrated that above urine flows of 2ml/min (augmentation limit), the
relationship between urea excretion and plasma concentration in any one
individual was constant, and expressed by a simple formu1a:
Curea = Uurea /
Purea
The term,
clearance, was introduced with this analysis. Since blood urea concentration is
frequently used as an index of filtration rate, it is worthwhile examining the
factors which influence it independently of intrinsic renal function. It has
alredy been pointed out that urine flow influences urea clearance. Urea
undergoes a complex intrarenal recycling process, the fractional reabsorption
increasing from 35% of the filtered load in hydrated states to 60% in dehydration.
The blood urea concentration is influenced by a variety of factors independent
of renal function. Changes in urine flow affect blood urea in a manner which
depends on the nephron segment where fluid is being reabsorbed.
Fig. 4
Fig. 5
The proximal
tubule is highly permeable to urea, and is the principal segment of passive
reabsorption. The distal nephron is less permeable to urea, even in the
presence of antidiuretic hormone. If ever ything else is left constant, salt
depletion will produce more azotemia at the same low rate of urine flow than
will water restriction, because salt depletion accelerates proximal
reabsorption while water restriction accelerates principally distal
reabsorption (12). Protein loads also influence blood urea concentration
independent of renal function. Figure 4 lists the sources of protein loads.
Factors 1-5 serve to increase protein loads while factor 6 reduces it. Figure 5
(13) illustrates the effect of protein intake at various levels of renal
function.
Fig. 6
It should be
emphasized that at low filtration rates, the BUN is very sensitive to protein
loads, as is illustrated by Figure 6 (13). Figure 7 summarizes the various
factors which influence both the BUN and urea clearance. It is evident that the
interpretation of the BUN as a rough index of GFR requires correction for the
numerous factors which influence its concentration independent of renal
function. Urea clearance circumvents some of the distorting effects of protein
loads. Nevertheless, it is always less than inulin clearance, but tends to rise
toward inulin clearance with advanced renal failure. These various factors are
discussed in detail in ref. 14.
Although Addis and
Van Slyke had published landmark studies on urea clearance as a measure of
renal function, the precise relation between urea clearance and glomerular
filtration rate was not appreciated. Rehberg (15, 16) introduced creatinine as
a marker of glomerular filtration rate, but was unaware that it was secreted by
the tubules, and therefore would give falsely high values, especially if its
plasma concentration was raised by infusions. Smith was skeptical that creatinine
would be an ideal marker for glomerular filtration, since it underwent
secretion in aglomerular fish, and might do the same in mammals, a supposition
that proved correct. He then went on to elaborate the criteria for an ideal
marker of GFR (Fig. 8).
Fig. 7
Fig. 8
The failure of
sugars to be secreted in aglomerular fish led Smith ultimately to identify
inulin as an ideal marker (17, 18). Simultaneously and independently, Richards
and his associates also demonstrated in micropuncture studies that inulin
fulfilled the requirements for an ideal marker of GFR (19). In Figure 9, inulin
excretion is shown to increase in direct proportion to its plasma concentration
when GFR is constant (a); inulin clearance is constant over a wide range of
plasma inulin concentrations (b); inulin clearance is constant over a wide
range of urine flows (c). Findings such as these established inulin as a kind
of gold standard for GFR (14). Smith went on to develop methods for measuring
renal blood flow, utilizing diodrast as a marker and the Fick principle to calculate
total renal blood flow. Since the Fick principle required renal vein
catheterization, it was unsuitable for routine use. Para-amino hippurate (PAH)
was identified as a substance which, at low plasma concentrations, was almost
completely secreted into the tubular urine. This eliminated the need for renal
catherization, since renal venous PAH could be assumed to be close to zero.
Subsequent studies of tubular maximum transport capacity using glucose and many
other substances provided a measure of functioning tubular mass.
Fig. 9
Fig. 10
These various
measures allowed Smith to portray the various functional aspects of normal and diseased
kidneys in remarkable detail, as summarized in his Porter lectures (20). From a
clinical and physiologic point of view, the various measures of renal function
that Smith and others explored over the years are summarized in Figure 10.
Smith has remarked how fruitful the clearance concept has proved to be. From
rather tentative beginnings it has stimulated the search for novel analytic
procedures, allowed for the assessment of renal function, and most of all
provided a conceptual rallying point for insight and understanding of renal
physiology.


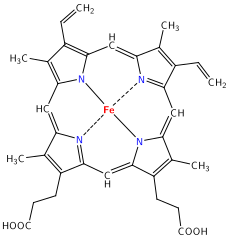{kind=link}

{kind=link}