INVESTIGATIONS OF LEUKOCYTES LABORATORY DIAGNOSIS OF LEUKEMIA’S
WHITE BLOOD CELL COUNT
The WBC count determines the number of leukocytes per
cubic millimeter of whole blood. The counting is performed very rapidly by
electronic devices. The WBC may be performed as part of a CBC, alone, or with
differential WBC count. An elevated WBC count is termed leukocytosis; a
decreased count, leukopenia. In addition to the normal physiological
variations in WBC count, many pathological problems may result in an abnormal
WBC count .

Causes of Altered White Blood Cell Differential by
Cell Type
|
Cell Type |
Increased Levels |
Decreased Levels |
|
Neutrophils |
Stress (allergies, exercise,
childbirth, surgery) Extremes of temperature Acute hemorrhage or hemolysis Infectious diseases Inflammatory disorders
(rheumatic fever, gout, rheumatoid arthritis,
drug reactions, vasculitis, myositis) Tissue necrosis (burns,
crushing injuries, abscesses Malignancies Metabolic disorders (uremia,
eclampsia, diabetic ketoacidosis, thyroid crisis, Cushing’s syndrome) Drugs (epinephrine, histamine,
lithium, heavy metals, heparin, digitalis, ACTH) Toxins and venoms (turpentine,
benzene) Leukemia (myelocytic) |
Bone marrow depression
(viruses, toxic chemicals, overwhelming infection, Felty’s syndrome, Gaucher’s
disease, myelofibrosis, hypersplenism, pernicious anemia, radiation) Anorexia nervosa, starvation,
malnutrition Folic acid deficiency Vitamin B12 deficiency Acromegaly Addison’s disease Thyrotoxicosis Anaphylaxis Disseminated lupus
erythematosus Drugs (alcohol, phenylbutazone [Butazolidin], phenacetin,
penicillin, chloramphenicol, streptomycin,
phenytoin [Dilantin], mephenytoin [Mesantoin], phenacemide
[Phenurone], tripelennamine [PBZ],
aminophylline, quinine, chlorpromazine,
barbiturates, dinitrophenols, sulfonamides, antineoplastics |
|
Bands |
Infections Antineoplastic drugs Any condition that causes
neutrophilia |
None, as bands should be
absent or present only in small numbers |
|
Basophils |
Leukemia Hodgkin’s disease Polycythemia vera Ulcerative colitis Nephrosis Chronic hypersensitivity
states |
None, as normal value is 0–1% |
|
Eosinophils |
Sickle cell disease Asthma Chorea Hypersensitivity reactions Parasitic infestations Autoimmune diseases Addison’s disease Malignancies Sarcoidosis Chronic inflammatory diseases
and dermatoses Leprosy Hodgkin’s disease Polycythemias Ulcerative colitis Autoallergies Pernicious anemia Splenectomy |
Disseminated lupus
erythematosus Acromegaly Elevated steroid levels Stress Infectious mononucleosis Hypersplenism Cushing’s syndrome Congestive heart failure Hyperplastic anemia Hormones (ACTH, thyroxine,
epinephrine) |
|
Monocytes |
Infections (bacterial, viral,
mycotic, rickettsial, amebic) Cirrhosis Collagen diseases Ulcerative colitis Regional enteritis Gaucher’s disease Hodgkin’s disease Lymphomas Carcinomas Monocytic leukemia Radiation Polycythemia vera Sarcoidosis Weil’s disease Systemic lupus erythematosus Hemolytic anemias Thrombocytopenic purpura |
Not characteristic of specific
disorders |
|
Lymphocytes |
Infections (bacterial, viral) Lymphosarcoma Ulcerative colitis Banti’s disease Felty’s syndrome Myeloma Lymphomas Addison’s disease Thyrotoxicosis Malnutrition Rickets Waldenström’s
macroglobulinemia Lymphocytic leukemia |
Immune deficiency diseases Hodgkin’s disease Rheumatic fever Aplastic anemia Bone marrow failure Gaucher’s disease Hemolytic disease of the
newborn Hypersplenism Thrombocytopenic purpura Transfusion reaction Massive transfusions Pernicious anemia Septicemia Pneumonia Burns Radiation Toxic chemicals (benzene,
bismuth, DDT) Antineoplastic agents Adrenal corticosteroids (high
doses) |

WHITE
BLOOD CELL COUNT
The WBC count determines the number of leukocytes per
cubic millimeter of whole blood. The counting is performed very rapidly by
electronic devices. The WBC may be performed as part of a CBC, alone, or with
differential WBC count. An elevated WBC count is termed leukocytosis; a decreased count, leukopenia. In addition to the normal
physiological variations in WBC count, many pathological problems may result in
an abnormal WBC count .
Causes of Altered White Blood Cell
Differential by Cell Type
|
Cell Type |
Increased
Levels |
Decreased
Levels |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Neutrophils |
Stress (allergies, exercise, childbirth, surgery) Extremes of temperature Acute hemorrhage or hemolysis Infectious diseases Inflammatory disorders (rheumatic fever, gout, rheumatoid arthritis, drug reactions, vasculitis, myositis) Tissue necrosis (burns, crushing injuries, abscesses Malignancies Metabolic disorders (uremia,eclampsia, diabetic ketoacidosis, thyroid
crisis, Cushing’s syndrome) Drugs (epinephrine, histamine, lithium, heavy metals, heparin,
digitalis, ACTH) Toxins and venoms (turpentine, benzene) Leukemia (myelocytic) |
Bone marrow depression (viruses, toxic chemicals, overwhelming
infection, Felty’s syndrome, Gaucher’s disease,myelofibrosis, hypersplenism, pernicious anemia, radiation) Anorexia nervosa, starvation, malnutrition Folic acid deficiency Vitamin B12 deficiency Acromegaly Addison’s disease Thyrotoxicosis Anaphylaxis Disseminated lupus erythematosus Drugs (alcohol, phenylbutazone [Butazolidin], phenacetin,
penicillin, chloramphenicol, streptomycin, phenytoin [Dilantin], mephenytoin [Mesantoin], phenacemide[Phenurone], tripelennamine [PBZ],
aminophylline, quinine, chlorpromazine, barbiturates,dinitrophenols,
sulfonamides,antineoplastics |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Bands |
Infections Antineoplastic drugs Any condition that causes neutrophilia |
None, as bands should be absent or present only in small numbers |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Basophils |
Leukemia Hodgkin’s disease Polycythemia vera Ulcerative colitis Nephrosis Chronic hypersensitivity states |
INVESTIGATIONS OF LEUKOCYTES LABORATORY DIAGNOSIS OF LEUKEMIA’S WHITE BLOOD CELL COUNT The WBC count determines the number of leukocytes per
cubic millimeter of whole blood. The counting is performed very rapidly by
electronic devices. The WBC may be performed as part of a CBC, alone, or with
differential WBC count. An elevated WBC count is termed leukocytosis; a
decreased count, leukopenia. In addition to the normal physiological
variations in WBC count, many pathological problems may result in an abnormal
WBC count .
Causes of Altered White Blood Cell Differential by
Cell Type
WHITE
BLOOD CELL COUNT The WBC count determines the number of leukocytes per
cubic millimeter of whole blood. The counting is performed very rapidly by
electronic devices. The WBC may be performed as part of a CBC, alone, or with
differential WBC count. An elevated WBC count is termed leukocytosis; a decreased count, leukopenia. In addition to the normal
physiological variations in WBC count, many pathological problems may result in
an abnormal WBC count . Causes of Altered White Blood Cell
Differential by Cell Type
LEUCOCYTES Leukocytes, or white
blood cells, are nucleated and are larger and less numerous than erythrocytes.
Leukocytes can be divided into 2 main groups, granulocytes and agranulocytes, according
to their content of cytoplasmic granules.
Each of these groups can
then be further divided on the basis of size, nuclear morphology, ratio of
nuclear to cytoplasmic volume, and staining properties. Two classes of
cytoplasmic granules occur in leukocytes, specific and azurophilic granules.
Specific granules are found only in granulocytes; their staining properties
(neutrophilic, eosinophilic, or basophilic) distinguish the 3 granulocytes
types. Azurophilic granules are
found in both agranulocytes and granulocytes. Azurophilic granules stain purple
and are lysosomes.
GRANULOCYTES Granulocytes have segmented nuclei and are described as
polymorphonuclear leukocytes (PMNLs). Depending on the cell type, the mature
nucleus may have from 2 to 7 lobes connected by thin strands of nucleoplasm.
Granulocyte types are most easily distinguished by their size and staining
properties, and by the appearance (as seen with an electron microscope) of the
abundant specific granules in their cytoplasm. These granules are all
membrane-limited and bud off the Golgi complex. All granulocytes have a life
span of a few days, dying by apoptosis (programmed cell death) in the
connoctive tissue. The resulting cellular removed by macrophages and does not
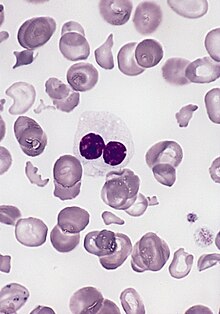
elicit an inflamatory response. Neutrophils – are the most abundant leukocytes in the blood. They
usually constitute 60-72 % of the white blood cells in healthy adults. They are
also found outside the bloodstream, especially in loose connective tissue.
Neutrophils are the first line of cellular defense against the invasion of
bacteria. Once they leave the bloodstream, they spread out, develop amoeboid
motility, and become active phagocytes. Unlike lymphocytes, neutrophils are all
terminally differentiated cells and so are incapable of mitosis. Size – neutrophils in the blood are approximately 12 μm in
diameter, while those in the tissues spread to a diameter of up to 20 μm. Nucleus – neutrophil nuclei contain highly condensed chromatin
both in the lobes and in the attenuated chromatin bridges between them. Most
have 3 lobes; however, lobe number increases from a single horseshoe-shaped
nucleus in immature neutrophils, called band neutrophils, to more than 5 lobes
in aging ones. The nuclei of certain diseased neutrophils, called
hypersegmented neutrophils, also have more than 5 lobes (they are typically old
cells). In females, a small heterochromatic body often extends from one of the
nuclear lobes. This represents the inactive X chromosome, or Barr body, and is
referred to as a drumstick – like appendage because of its characteristic
shape.
Neutrophil cytoplasm is abundant and filled with specific membrane-bound
granules. These granules are modified lysosomes and have a bacteriocidal
function. Azurophilic granules (primary, or type A) stain with azure dye and
are diagnostic for neutrophils. These large (0.4 um) electron-dense granules
comprise about 20 % of the granule population and are visible in the light
microscope. Specific granules (secondary, or type B)
are smaller (0.2 μm) and may contain crystalloids. They comprise 80 % of
the granule population and are not visible in the light microscope. They stain
salmon pink with typical bloodstains. The less numerous azurophilic granules
stain a reddish-purple. The specific granules contain alkaline phosphatase and
bactericidal cationic proteins called phagocytins. Azurophilic granules contain
lysosomal enzymes and peroxidase. Neutrophils also contain more glycogen than
other leukocytes. Neutrophils are short-lived cells with a half-life of 6-7 hours in
blood and a life span of 1-4 days in connective tissues, where they die by
apoptosis. The primary function of neutrophils is the phagocytosis and
destruction of bacteria. Neutrophils are active phagocytes of small particles
and have sometimes been called microphages to distinguish them from
macrophages, which are larger cells. Neutrophils are inactive and spherical
while circulating but change shape upon adhering to a solid substrate, over
which they migrate via pseudopodia. Bacteria first adhere to the neutrophil surface and then are
surrounded and engulfed by pseudopodia; in this way bacteria eventually occupy
vacuoles (phagosomes) delimited by a membrane derived from the cell surface.
Immediately thereafter, specific granules fuse with and discharge their
contents into the phagosomes. Azurophilic granules then discharge their enzymes
into the acid environment, killing and digesting the microorganisms. The mechanism of phagocytosis Phagocytosis – is active devourment of the solid substances by cells. Cells, which
are capable of phagocytosis, are called phagocytes. There are poly phagocytes
(neutrophils) and mononuclear phagotyces (monocytes). Phagocytes must be
selective of the material that is phagocytized; otherwise, normal cells and
structures of the body might be ingested. Whether phagocytosis will occur,
depends especially on three selective procedures. Firstly, most natural
structures in the tissues have smooth surfaces, which resist phagocytosis. But
if the surface is rough, the likelihood of phagocytosis is increased. Secondly,
most natural substances of the body have protective protein coats that repel
the phagocytes. Conversely, most dead tissues and foreign particles have no
protective coats, which make them subject to phagocytosis. Thirdly, the immune
system of the body develops antibodies against infectious agents such as
bacteria. The antibodies then adhere to the bacterial membranes and thereby
make the bacteria especially susceptible to phagocytosis. To do this, the
antibody molecule also combines with the C3 product of the complement cascade, which is an additional part of the
immune system discussed in the next chapter. The C3 molecules, in turn, attach
to receptors on the phagocytic membrane, thus initiating phagocytosis. This
selection and phagocytosis process is calledopsonization.
Stages of phagocytosis: I Conjugation stage. Phagocyte moves to direction of not self agent (chemotaxis). II Adhesion stage. Phagocyte interacts with the agent. There are two mechanisms: 1) without
receptor: electrostatic and hydrophobic interaction (phagocyte is negatively
charged, positive particles); 2) with
receptor. On the surface of macrophages there are receptors for
opsonin-substances that can interact with bacteria. III Devourment stage. Its steps: · invagination
of phagocyte membrane on the contact place; · the formation
of phagosome, which contains the agent; · the formation
of phagolysosome: consolidation of phagosome with lysosomes (secondary
granules). IV Digestive stage. Its steps: · The disposal of bacteria –
intercellular cytolysis with the help of germicide systems of phagocytes
(myeloperoxidase system, which produces hypochloride ion ClO-, free
radicals and peroxides O30, HO20, OH0,
lisocim, lactoferin, non-enzymatic cationic proteins, lactic acid). · Digestion – hydrolysis of killed
bacteria with the help of hydrolytic enzymes. Eosinophils – constitute only 0,5-54
% of the circulating leukocytes in healhty adults. They may leave the
bloodstream by diapedesis, spread out, and move about in the connective
tissues. They are capable of only limited phagocytosis, showing a preference
for antigen-antibody complexes. The number of circulating eosinophils typically
increases (eosinophilia) during allergic reactions and in response to parasitic
(helmintic) infections, and rapidly decreases in response to treatment with
exogenous corticosteroids. These cells produce substances that modulate
inflammation by inactivating the leukotriens and histamine produced by other
cells.
Basophils vary in
diameter from 12 μm
to 15 μm but are usually
slightly smaller than neutrophils. Their nuclei are less heterochromatic than
other granulocytes and usually consist of 3 irregular lobes which are often
obscured by the large, dark-staining cytoplasmic granules. The specific granules
of basophils are their most characteristic feature. These granules have
irregular shapes and vary in size; the largest are the size of the specific
granules of eosinophils, the smallest nearly as small as those of neutrophils.
The granules stain metachromatically and appear reddish-violet to nearly black
in stained blood smears. The specific granules of basophils (like those of the
mast cells of connective tissue) contain heparin and histamine, which may be
released by exocytosis in response to certain types of antigenic stimuli. The
granules may contain inclusions, but they appear more homogeneously
electron-dense than do those of eosinophils.
Functions. Basophils mediate the inflammatory response and secrete eosinophil
chemotactic factor. In response to certain antigens, basophils stimulate the
formation of immunoglobulin E(IgE)-a class of
antibodies. Subsequent exposure to the same antigen can cause a basophil and
mast cell response restricted to specific organs (e.g., bronchial asthma in the
lungs or a severe and systemic response such as anaphylactic shock brought on
by a bee sting). Agranulocytes Agranulocytes have round
unsegmented nuclei and are described as mononuclear leukocytes. They lack
specific granules, but they contain various number of azurophilic granules
(lysosomes) that bind the azure dies of the stain. This group includes the
lymphocytes and monocytes. Lymphocytes – constitute
a diverse class of cells; they have similar morphologic characteristics but a
variety of highly specific functions. They normally account for 20-25 % of the
white blood cells in adult blood, with a considerable range of normal variation
(20-45%). Lymphocytes are also found outside the blood vessels, grouped in
lymphatic organs or dispersed in connective tissues. They respond to invasion
of the body by foreign substances and organisms and assist in their
inactivation. They also have diverse functional roles, all related to immune
reactions in defending against invading microorganisms, foreign macromolecules
and cancer cells. Unlike other leukocytes, lymphocytes never become phagocytic.
They can be classified into several groups due to distinctive surface
molecules (markers), which can be distinguished only by immunocytochemical
methods. The 2 major functional classes of lymphocytes are T cells and B cells.
Lymphocytes in the blood are predominantly (about 80 %) T
cells.
Lymphocytes vary from 6
to 18 μm in diameter. Most of those found in blood are small lymphocytes
in the 6- to 8 μm range, making them the smallest leukocytes, comparable
in size to erythrocytes. A small number of medium-sized and large lymphocytes
are also ground in the circulation and probably represent lymphocytes activated
by an antigen. Lymphocyte nuclei
are spheric and often flattened on one side. In small lymphocytes, the nucleus
is densely heterochromatic, staining purplish-blue to black, and nearly fills
the cell. In large lymphocytes, the nucleus is larger and less dense and stains
reddish-purple. Lymphocyte
cytoplasm exhibits a pale basophilia and occasionally contains a few purplish
azurophilic granules but lacks specific granules. In the smaller cells, the
cytoplasm forms a thin rim around the nucleus; in the larger cells, it is more
abundant. It contains many free ribosomes, few mitochondria, sparse endoplasmic
reticulum, and a small Golgi complex. When stimulated by an antigen,
lymphocytes undergo blast transformation, a process of enlargement and
sequential mitotic divisions. Some of the daughter cells, called memory cells,
return to an inactive state but retain the capacity to respond more quickly to
the next encounter with the same antigen. Other daughter cells, called effector
cells, become activated to carry out an immune response to the antigen.
Effector cells may be derived from either B lymphocytes (B cells) or T
lymphocytes (T cells). While circulating B and T cells are morphologically
indistingushable, they carry different cell-surface components (antigens
recognized by other species) and can be identified by special procedures. B Lymphocytes
differentiate into plasma cells, which secrete specific antigen-binding
molecules (antibodies or immunoglobulins) that circulate in the blood and lymph
and serve as a major component of humoral immunity. T Lymphocyte derivatives serve as the major cells of the
cellular immune response. They produce a variety of factors, termed lymphokines
(eg, interferon) that influence the activities of macrophages and of other
leukocytes involved in an ammune response. There are several types: (I) Cytotoxic
(killer) cells secrete substances that kill other cells and in some cases kill
by direct contact; they play the major role in graft rejection. (II) Helper T cells
enhance the activity of some B cells and other T cells. (III) Suppressor T
cells inhibit the activity of some B cells and other T cells. The primary (central)
lymphoid organs include the thymus, where lymphocyte precursors are programmed
to become T cells and, in birds, the bursa of Fabricius, where lymphocyte
precursors are programmed to become B cells. Humans have no bursa; our B cells
appear to be programmed in the bone marrow. According to the electron-microscopic
studies there are 4 different types: 1. Small dark
lymphocytes; 2. Small light
lymphocytes; 3. Medium lymphocytes; 4. Plasmocytes or
lymphoplasmocytes. Lymphocytes vary in life span; some
live only a few days, and others survive in the circulating blood for many
years. Lymphocytes are the only type of leukocytes that return from tissue back
to the blood, after diapedesis. Monocytes are often confused with large
lymphocytes, but they are larger and constitute only 3-8 % of the white blood
cells in healthy adults. Monocytes are found only in the blood, but they remain
in circulation for less than a week before migrating through capillary walls to
enter other tissues or to become incorporated in the lining of sinuses. Once outside
the bloodstream, they become phagocytic and apparently do not recirculate.
Monocytes are the direct precursors to macrophages. The mononuclear phagocyte
system (portions of which were formerly referred to as
the reticuloendothelial system) consists of monocyte-derived phagocytic cells
distributed throughout the body. Examples include the Kupffer cells of the
liver and some of the macrophages of connective tissues.
Monocytes in the blood of
healthy adults have a diameter of 12-15 μm, but when they attach to
surfaces they flatten and spread out, often reaching 20 μm in diameter
they are the largest among leukocytes). Monocyte nuclei may
be ovoid, but are usually kidney- or horseshoe shaped and eccentrically placed;
unlike lymphocyte nuclei, they are rarely spherical. The chromatin is less
condensed than that of lymphocyte nuclei, has a “smudgy” appearance, and stains
reddish-purple. There may be 2-3 nucleoli, but these are often difficult to
distinguish. Cytoplasm – The faint
blue-gray cytoplasm of monocytes is more abundant than that of lymphocytes and
contains many small azurophilic granules, which are distributed through the
cytoplasm, giving it a bluish-gray color in stained smears. In the lectrone
microscope, one or two nucleoli are seen in the nucleus, and a small quantity
of rough endoplasmic reticulum, polyribosomes. It also contains many small
mitochondria, a well-developed Golgi apparatus. Many microvilli and pinocytotic
vesicles are found at the cell surface. An increase in the
number of leukocytes is called leukocytosis; this occurs in most systemic and
localized infectious processes, such as appendicitis or abscesses. It is a
normal response to infection. On the other hand, a decrease in the number of
leukocytes is called leukopenia; this may occur in certain acute and chronic
diseases, such as typhoid fever or tuberculosis. Leukopenia is also a constant
finding in radiation sickness, the clinical result of excessive exposure to
gamma rays. For example, victims of the atomic bomb expositions were exposed to
intensive radiation and as result suffered a marked depression of bone marrow
function; the absolute white count in the more severe cases ranged from 1500 to
zero per cu. mm. of blood. There also was anemia, due to interference with formation
of red blood cells. Life of white blood cells Lifespan of white blood cells are not constant. It depends upon the demand in the body and their function. Lifespan
of these ceils may be as short as half a day or it may be as long as 3-6 months. However, the normai lifespan of
white biood cells is as follows: Neutrophils — 2-5 days Eosinophils — 7-12 days Basophils — 12-15 days Monocytes — 2-5 days Lymphocytes — 1/2-1 day The amount in peripheral blood – 4-9
· 109/liter. The decrease of leucocytes amount is
called leucopenia, the increase – leucocytosis. There are 2 types of
leucocytes: V Physiological – is normal, physiological reaction of
the organism in some irritations. There are following types, dependently on
their causes: 1) emotional
leucocytosis (occurs in result of emotional stresses); 2) myogenic
(occurs in result of intensive physical exercises); 3) static
(occurs in result of change of the position of the human body from horizontal
to vertical); 4) alimental
(occurs during or after eating); 5) painful
(occurs during strong painful feelings); 6) leucocytosis
of pregnant; 7) leucocytosis
of newborn. II Pathological (reactive)
– it is connected with the pathological process in the organism. Its reasons: 1)
infectious diseases; 2)
inflammatory processes; 3)
allergic reactions; 4) intoxications of endo- and exogenous origin. The difference
between physiological and reactive leucocytosis Physiological
leucocytosis: 1) it
is redistributing (leucocytes from the parietal pool are moving into
circulation); 2) it
has transient character (it is normalizing fast after the cause disappears); 3) leukogram
does not change (the correlation between different forms persists); 4) degenerative
forms of leucocytes do not appear. Reactive
leucocytosis is connected with the increase of proliferation and maturating of
leucocytes in red bone marrow or increase of moving of reserve leucocytes from
RBM to the blood. During pathological leucocytosis the correlation between
different forms of leucocytes is disturbed. Percentage ratio between
different forms of leucocytes is called leukogram (formula of Arnet-Shilling). Differential white blood cell count (Differential
leukocyte count) Physiological values
of leukocyte count: 5-10 x 109/L blood Neutrophil
granulocytes Physiological values:
2-7.5 x 109/l (60-70%) Increased number -
neutrophilia: bacterial infections, trauma, scorch, bleeding, inflamations,
infarction, polymialgy, myeloproliferative disorders, reaction to certain
medications (e.g. chorticosteroides). Significantly increased in leukemia,
disseminated malignant diseases and complicated childhood infections. Decreased number -
neuthropenia: viral infections, brucellosis, thyphoid, Kala-azar, TBC, sepsis,
lupus erithematodes, rheumatoid arthritis, avitaminosis B12 i bone marrow dissorders. Medications
like carbamazepine or sulphonamides can decrease a number of
neuthrophils. Band neutrophils (stab
neutrophils) cells are younger forms of cells presented with kidney-shape,
curved nucleus and not segmented, lobar nucleus. Usually they are represent
3-5% of leukocytes. Increased value indicates a higher demand and expenditure
of neutrophils, and is called “left shift” (referring to ratio of immature to
mature forms of neutrophils). Lymphocytes Physiological values:
1.3-3.5 x 109/l (20-40%). Increased number -
lymphocytosis: viral infections (EBV-Epstein Barr virus, CMV-cytomegalovirus,
rubeola), toxoplasmosis, pertusis, brucellosis, chronic lymphatic leukemia. Decreased number -
lymphopenia: corticosteroid treatment, lupus erithematodes, uremia, legionella
disease, AIDS, bone marrow
infiltration (tumor), after chemotherapy and radiotherapy. Subclases: CD4: 537-1571/mm3 (decreased
in HIV infection); CD8: 235-753/mm3; CD4/CD8 ratio: 1.2-3.8. Eosinophil
granulocytes Physiological values:
0.04-0.44 x 109/l (1-4%). Increased number -
eosinophilia: asthma i allergic disease, parasitic infestations, skin diseases
(especially pemphigus), urticaria, egzema, malignant diseases (including
eosinophilic leukemia), irradiation, Loeffler syndrome, recovery after
infections. Hypereosinophilic syndromecan be observed in terminal organ damage
(restrictive cardiomyopathy, neuropathy, hepatosplenomegaly), withincreased
eosinophile number for more than 6 weeks (>1.5 x 109/l). Eosinophilia-myalgi
syndrome – muscle pain (myalgia), joint pain (arthralgia), increased body
temperature, rash, arms swelling and intense eosinophilia. Monocytes Physiological values:
0.2-0.8 x 109/l (2-6%). Increased number -
monocytosis: acute and chronic infection (TBC, brucellosis, protozoal
infections), malignant diseases (acute myeloid leukemia, Hodgkin lymphoma),
myelodisplasia. Basophil granulocytes Physiological values:
0.01 x 109/l (0.5-1%). Increased number -
basophilia: viral infections, urticaria, myxedema, after splenectomy, chronic
myeloid leukemia, malignant disease, systemic mastocytosis (urticaria
pigmentosa), hemolysis, policitemia rubra vera. Healthy human has instant white
blood cell count and any changes in it – is the signal to different sicknesses. The
disturbance in correlation between immature and mature forms of neutrophils is
called shift of leukogram. There is shift to the left and shift to the right. Shift to the left is
characterized byincrease in the content of immature neutrophils. Myelocytes
appear in blood, the amount of metamyelocytes increase. This happens during
leucocytosis. Shift to the right is
characterized with domination of mature neutrophils with big amount of segment
(5-6) on the background of disappearance of immature forms. This testifies the
development of inflammatory process.
Production of
leucocytes Granulopoiesis The maturation process of
granulocytes takes place with cytoplasmic changes characterized by the
synthesis of a number of proteins that are packed in two organelles: the
azurophilic and specific granules. These proteins are produced in the rough
endoplasmic reticulum and the Golgi complex in two successive stages. The first
stage results in the production of the azurophilic granules. In the second
stage, a change in synthetic activity takes place with the production of
several proteins that are packed in the specific granules. These granules
contain different proteins in each of the three types of granulocytes and are
utilized for the various activities of each type of granulocyte. Maturation of
Granulocytes The myeloblast is the
most immature recognizable cell in the myeloid series. It has a finely
dispersed chromatin, and nucleoli can be seen. In the next stage, the
promyelocyte is characterized by its basophilic cytoplasm and azurophilic
granules. These granules contain lysosomal enzymes and myeloperoxidase. The promyelocyte gives
rise to the three known types of granulocyte. The first sign of differentiation
appears in the myelocytes, in which specific granules gradually increase in
quantity and eventually occupy most of the cytoplasm. These neutrophilic,
basophilic, and eosinophilic myelocytes mature with further condensation of the
nucleus and a considerable increase in their specific granule content. Kinetics of Neutrophil
Production The total time taken for
a myeloblast to emerge as a mature neutrophil in the circulation is about 11
days. Under normal circumstances, five mitotic divisions occur in the
myeloblast, promyelocyte, and neutrophilic myelocyte
stages of development. Neutrophils pass through
several functionally and anatomically defined compartments: 1- The medullary formation compartment
can be subdivided into a mitotic compartment (≈3 days) and a maturation
compartment (≈4 days). 2- A medullary storage compartment.
Neutrophils remain in this compartment for about 4 days. 3- The circulating compartment consists
of neutrophils suspended in plasma and circulating in blood vessels. 4- The marginating compartment is
composed of neutrophils that are present in blood but do not circulate. These
neutrophils are in capillaries and are temporarily excluded from the
circulation by vasoconstriction, or—especially in the lungs—they may be at the
periphery of vessels, adhering to the endothelium, and not in the main
bloodstream. The marginating and
circulating compartments are of about equal size, and there is a constant
interchange of cells between them. The half-life of a neutrophil in these two
compartments is 6–7 h. The medullary formation and storage compartments
together are about 10 times as large as the circulating and marginating
compartments. Neutrophils and other
granulocytes enter the connective tissues by passing through intercellular
junctions found between endothelial cells of capillaries and postcapillary
venules (diapedesis). The connective tissues form a fifth compartment for
neutrophils, but its size is not known. Neutrophils reside here for 1–4 days
and then die by apoptosis, regardless of whether they have performed their
major function of phagocytosis. Maturation of Lymphocytes
& Monocytes Study of the precursor
cells of lymphocytes and monocytes is difficult, because these cells do not
contain specific cytoplasmic granules or nuclear lobulation, both of which
facilitate the distinction between young and mature forms of granulocytes.
Lymphocytes and monocytes are distinguished mainly on the basis of size,
chromatin structure, and the presence of nucleoli in smear preparations. Lymphocytes Circulating lymphocytes
originate mainly in the thymus and the peripheral lymphoid organs (eg, spleen,
lymph nodes, tonsils). However, all lymphocyte
progenitor cells originate in the bone marrow. Some of these lymphocytes
migrate to the thymus, where they acquire the full attributes of T lymphocytes.
Subsequently, T lymphocytes populate specific regions of peripheral lymphoid
organs. Other bone marrow lymphocytes differentiate into B lymphocytes in the
bone marrow and then migrate to peripheral lymphoid organs, where they inhabit
and multiply in their own special compartments. The first identifiable
progenitor of lymphoid cells is the lymphoblast, dividing two or three times to
form prolymphocytes. Monocyte The monoblast is a
committed progenitor cell that is almost identical to the myeloblast in its
morphological characteristics. Further differentiation leads to the
promonocyte, a large cell (up to 18 µm in diameter) with a basophilic cytoplasm
and a large, slightly indented nucleus. The chromatin is lacy, and nucleoli are
evident. Promonocytes divide twice in the course of their development into
monocytes. A large amount of rough endoplasmic reticulum is present, as is an
extensive Golgi complex in which granule condensation can be seen to be taking
place. These granules are primary lysosomes, which are observed as fine
azurophilic granules in blood monocytes. Mature monocytes enter the
bloodstream, circulate for about 8 h, and then enter the connective tissues,
where they mature into macrophages and function for several months. Origin of Platelets In adults, platelets
originate in the red bone marrow by fragmentation of the cytoplasm of mature
megakaryocytes,which, in turn, arise by
differentiation of megakaryoblasts. Megakaryoblasts The megakaryoblast is
15–50 µm in diameter and has a large ovoid or kidney-shaped nucleus with
numerous nucleoli. The nucleus becomes highly polyploid (ie, it contains up to
30 times as much DNA as a normal cell) before platelets begin to form. The
cytoplasm of this cell is homogeneous and intensely basophilic Megakaryocytes The megakaryocyte is a
giant cell (35–150 µm in diameter) with an irregularly lobulated nucleus,
coarse chromatin, and no visible nucleoli. The cytoplasm contains numerous
mitochondria, a well-developed rough endoplasmic reticulum, and an extensive
Golgi complex. Platelets have conspicuous granules, originating from the Golgi
complex, that contain biologically active substances, such as platelet-derived
growth factor, fibroblast growth factor, von Willebrand's factor (which
promotes adhesion of platelets to endothelial cells), and platelet factor
IV(which stimulates blood coagulation). CLINICAL LABORATORY DIAGNOSTICS OF HEMOBLASTOSIS Etiology is Unknown: Possible Causes: B.
Marrow damage due to irradiation increases the frequency of some leukemias, but not others. D.
Possible genetic factors have been implicated, especially in
Chronic Lymphocytic Leukemia. 2. If the prominent
cell line is of the lymphoid series it is a lymphocytic leukemia Therefore,
there are four basic types of leukemia. II. Acute
lymphocytic leukemia – ALL - (includes T cell, B cell, and Null cell) III. Chronic
myelocytic leukemia – CML - (includes myelocytic and myelomonocytic) Acute
leukemias can occur in all age groups n ALL is more common in children n AML is more
common in adults Chronic
leukemias are usually a disease of adults n CLL is
extremely rare in children and unusual before the age of 40 Age
Distribution: optimum ages
for development: 5.
Monocytic: middle age (rarely
before 30) Comparison of
acute and chronic leukemias: Clinical
onset sudden insidious Course
(untreated) 6 mo. or less
2-6 years Leukemic
cells immature >30%
blasts more mature cells Thrombocytopenia prominent mild Lymphadenopathy mild present; often
prominent Splenomegaly mild present; often
prominent Malignant
transformation of a stem cell leading to unregulated proliferation and
Pathophysiology
of the clinical manifestations of acute leukemias 1. Marrow
failure due to infiltration -thrombocytopenia -bleeding,
spontaneous bruising -neutropenia-infections, sepsis 2. Infiltration of other organs -liver,
spleen, lymph nodes (particularly in ALL) -gums –gum hypertrophy (monocytic subtype of AML) -bone pain,
esp. in children with ALL 3.
Leukostasis (only seen with WBC >>50x109 /L) -lungs -pulmonary infiltrates, hypoxemia -exposure of
substances that can initiate coagulation can cause DIC The lab
diagnosis is based on two things: 2.
Identification of the cell lineage of the leukemic cells Anemia (normochromic, normocytic) The degree of
peripheral blood involvement determines classification: n Leukemic –
increased WBCs due to blasts n
Subleukemic –
blasts without increased WBCs n Aleukemic –
decreased WBCs with no blasts Classification
of the immature cells involved may be done by:
Myeloblast with
auer rods Lymphoblasts
Auer rods in AML Cytochemistry Cytochemistry
– help to classify the lineage of a leukemic cell (myeloid versus lymphoid). Myeloperoxidase
– is found in the primary granules of granulocytic cells starting at the late
blast stage. Monocytes may be weakly
positive.
Sudan black stains phospholipids, neutral fats and
sterols found in primary and secondary granules of granulocytic cells and to a
lesser extent in monocytic lysosomes.
Rare positives occur in lymphoid cells. Nonspecific esterase – is used to
identify monocytic cells which are diffusely positive. T lymphocytes may have focal staining.
Acid phosphatase may be found in myeloblasts and
lymphoblasts. T lymphocytes have a high level of acid phosphatase and this can
be used to help make a diagnosis of acute T-lymphocytic leukemia.
Leukocyte alkaline phosphatase – is located in
the tertiary granules of segmented neutrophils, bands and metamyelocytes. The
LAP score is determined by counting 100 mature neutrophils and bands. Each cell
is graded from 0 to 5. The total LAP score is
calculated by adding up the scores for each cell.
Chronic
Lymphocytic Leukemia Neoplastic proliferation of small mature-appearing lymphocytes >99 % are B-cell derived Older patients (> 40) Disease may be discovered incidentally Fatigue, weakness, weight loss, anorexia, and/or recurrent infections
may occur Variable splenomegaly and non tender lymphadenopathy Leukemic counterpart of small lymphocytic Lymphoma Malignant
transformation of a stem cell leading to unregulated proliferation and tissue with lesion of
lymph nodes and organs, characterized by growth of the giant cells called
Reed-Sternberg- Beresovsky cells, large and small atypical cells (Hodgkin,s
cells) and inflammatory infiltration.
Hodgkin disease: a giant
mononuclear cell with a large nucleolus (arrow) and wide cytoplasmic layer
(Hodgkin cell), surrounded by small and medium-sized lymphocytes. Hodgkin disease: giant binuclear
cell (Reed–Sternberg giant cell). Hodgkin's
lymphoma, also known as Hodgkin lymphoma and previously known as Hodgkin's disease, is a type of lymphoma, which is a cancer originating from white blood cells called lymphocytes. Patients with Hodgkin's
lymphoma may present with the following symptoms: §
Lymph nodes:
the most common symptom of Hodgkin's is the painless enlargement of one or more
lymph nodes, or lymphadenopathy. The nodes may also feel rubbery and swollen when examined. The nodes
of the neck and shoulders (cervical and supraclavicular) are most frequently involved (80–90 % of the time, on average). The
lymph nodes of the chest are often affected, and these may be noticed on
a chest radiograph. §
Unexplained weight loss §
Splenomegaly: enlargement of the spleen occurs
in about 30 % of people with Hodgkin's lymphoma. The enlargement, however, is
seldom massive and the size of the spleen may fluctuate during the course of
treatment. §
Hepatomegaly: enlargement of the liver,
due to liver involvement, is present in about 5 % of cases. §
Hepatosplenomegaly: the enlargement of both the liver and spleen caused by the same
disease. § Red-coloured patches on the skin, easy bleeding and petechiae due to low platelet count (as a result of
bone marrow infiltration, increased trapping in the spleen etc. – i.e.
decreased production, increased removal) the syringe. The syringe body is separated from the needle
and the mandrel Cell composition
in the bone marrow: normal values (%)
Squash
preparation and meandering smear for the cytological analysis of bone marrow
spicules
Bone Marrow:
Medullary Stroma Cells
|