Investigation of thyroid hormones in the regulation of
metabolism. Hormonal regulation of
calsium and phosphorus homeostasis.
Tissue hormones. Investigation of molecular – cellular
mechanisms of adrenal and sex glands hormones.
Hormones of thyroid and parathyroid,
structure, mechanism of action.
Thyroid synthesizes two kinds of hormones: iodine
containing hormones and calcitonin.
Iodine containing hormones - thyroxine and
triiodthyronine.
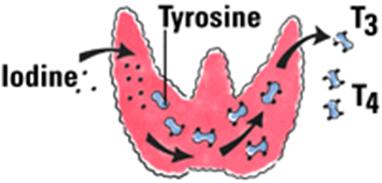
Thyroxine and triiodthyronine are iodinated derivatives
of amino acid tyrosine.

Functions: these hormones are necessary for growth of
organism, mental, physical and sex development, they regulate the rate of basal
metabolism.
http://www.youtube.com/watch?v=2AFiMipv63k&feature=related
Effect of thyroxine and
triiodthyronine on the protein metabolism:
1. in normal concentration
stimulate the synthesis of proteins and nucleic acids;
2.
in excessive concentration activate the catabolic
processes.
Effect of thyroxine and
triiodthyronine on the carbohydrate metabolism:
1. promote the
absorption of carbohydrates in the intestine;
2. activates the
decomposition of glycogen.
Effect of thyroxine and
triiodthyronine on the lipid metabolism:
-
activate the lipid oxidation and mobilization.
Effect of thyroxine and
triiodthyronine on the energy metabolism:
1. activates
dehydrogenases of mitochondria;
2. in excessive
amount of these hormones the disconnection of tissue respirstion and oxidative
phosphorylation takes place. As result the formation of ATP is decreased and
the temperature of the organism is increased.
Excessive secretion of thyroid hormones, called hyperthyroidism,

is responsible for Graves'
disease,
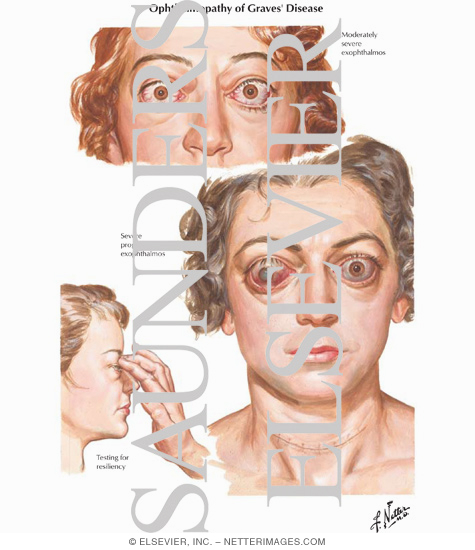
,
or exophthalmic goiter

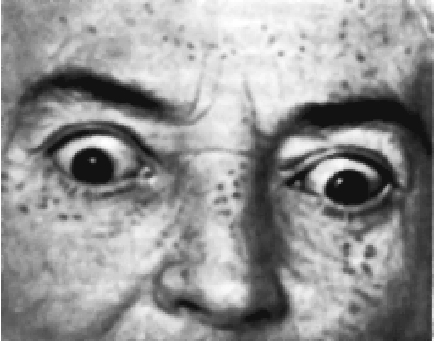
exophthalmic goiter
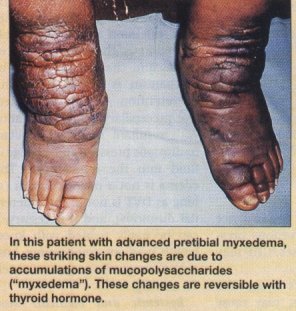
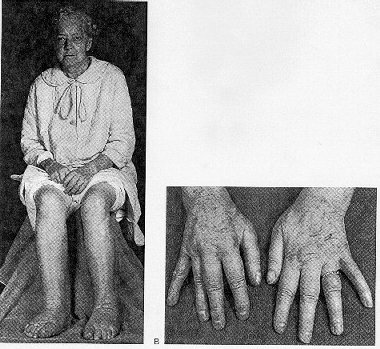
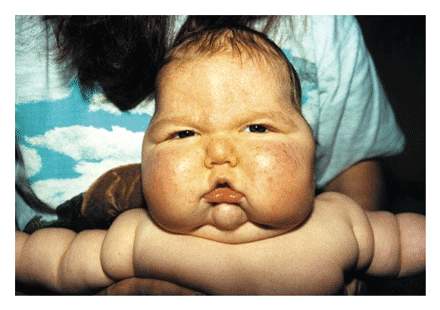
while deficiency in thyroid hormones, hypothyroidism
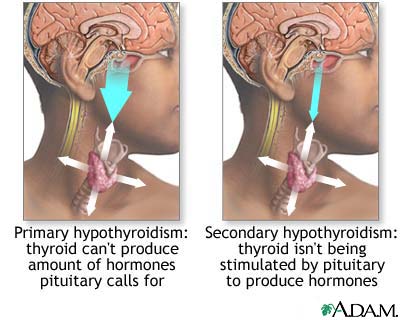
is characteristic of the disease myxedema.
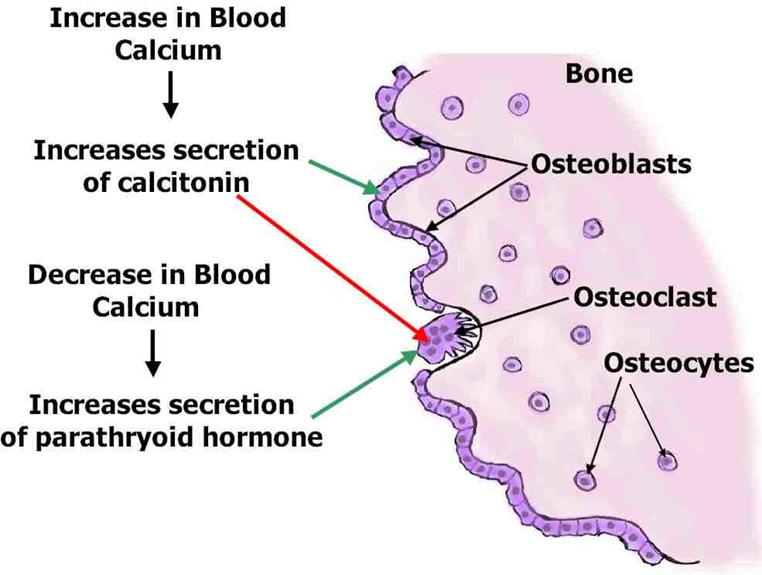
Calcitonin.
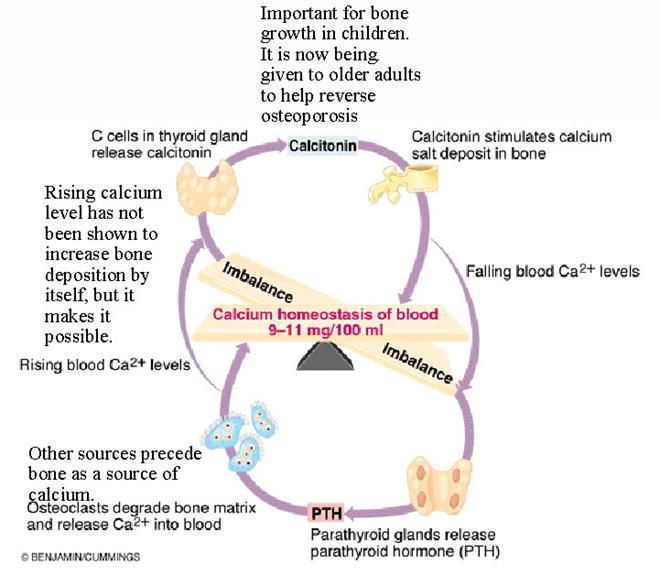
Calcitonin is synthesized by the parafollicle
cells of thyroid.
Chemical structure: peptide.
Functions: - promotes the transition of calcium from
blood in bones;
-
inhibits the reabsorption of phosphorus in
kidneys.
Thus, calcitonin decreases the Ca and P contents in
blood.
Parathyroid glands.
Parathyroid hormone. Chemical structure: protein.
Functions:
1.
promotes the transition of calcium from bones to blood;
2.
promotes the absorption of Ca in the intestine;
3.
inhibits the reabsorption of phosphorus in kidneys.
Thus,
parathyroid hormone increases the Ca amount in blood and decreases the P amount in blood.
Body Distribution of Calcium and Phosphate
There are three major pools of calcium in the body:
- Intracellular
calcium:
- A large
majority of calcium within cells is sequestered in mitochondria and
endoplasmic reticulum. Intracellular free calcium concentrations fluctuate
greatly, from roughly 100 nM to greater than 1 uM, due to release from
cellular stores or influx from extracellular fluid. These fluctuations are
integral to calcium's role in intracellular signaling, enzyme activation
and muscle contractions.
- Calcium
in blood and extracellular fluid:
- Roughly
half of the calcium in blood is bound to proteins. The concentration of
ionized calcium in this compartment is normally almost invariant at
approximately
- Bone
calcium:
- A vast
majority of body calcium is in bone. Within bone, 99% of the calcium is
tied up in the mineral phase, but the remaining 1% is in a pool that can
rapidly exchange with extracellular calcium.
As with calcium, the majority of body phosphate (approximately 85%) is
present in the mineral phase of bone. The remainder of body phosphate is
present in a variety of inorganic and organic compounds distributed within both
intracellular and extracellular compartments. Normal blood concentrations of
phosphate are very similar to calcium.
Fluxes of Calcium and Phosphate
Maintaining
constant concentrations of calcium in blood requires frequent adjustments,
which can be described as fluxes of calcium between blood and other body
compartments. Three organs participate in supplying calcium to blood and
removing it from blood when necessary:
- The small
intestine is the site where dietary calcium is absorbed. Importantly,
efficient absorption of calcium in the small intestine is dependent on
expression of a calcium-binding protein in epithelial cells.
- Bone serves as a vast reservoir of
calcium. Stimulating net resorption of bone mineral releases calcium and
phosphate into blood, and suppressing this effect allows calcium to be
deposited in bone.
The kidney
is critcally important in calcium homeostasis. Under normal blood calcium
concentrations, almost all of the calcium that enters glomerular filtrate is
reabsorbed from the tubular system back into blood, which preserves blood
calcium levels. If tubular reabsorption of calcium decreases, calcium is lost
by excretion into urine.
Hormonal Control Systems
Maintaining normal blood calcium and phosphorus concentrations is
managed through the concerted action of three hormones that control fluxes of
calcium in and out of blood and extracellular fluid:
Parathyroid hormone serves to increase blood
concentrations of calcium. Mechanistically, parathyroid hormone preserves blood calcium by several
major effects:
- Stimulates
production of the biologically-active form of vitamin D within the kidney.
- Facilitates
mobilization of calcium and phosphate from bone. To prevent detrimental
increases in phosphate, parathyroid hormone also has a potent effect on
the kidney to eliminate phosphate (phosphaturic effect).
- Maximizes
tubular reabsorption of calcium within the kidney. This activity results
in minimal losses of calcium in urine.
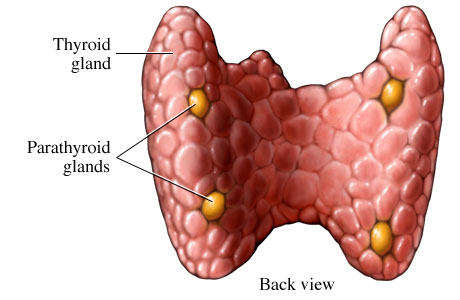
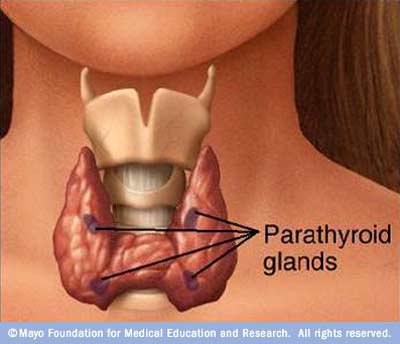
Parathyroid Gland
Four small masses of epithelial tissue are embedded in the connective
tissue capsule on the posterior surface of the thyroid glands. These are
parathyroid glands, and they secrete parathyroid hormone or parathormone.
Parathyroid hormone is the most important regulator of blood calcium levels.
The hormone is secreted in response to low blood calcium levels, and its effect
is to increase those levels.
Hypoparathyroidism, or insufficient secretion of parathyroid hormone,
leads to increased nerve excitability. The low blood calcium levels trigger
spontaneous and continuous nerve impulses, which then stimulate muscle
contraction.
Since parathyroid gland disease (hyperparathyroidism) was first
described in 1925, the symptoms have become known as "moans, groans,
stones, and bones...with psychic overtones". Although about 5-7% of people with parathyroid disease
(hyperparathyroidism) claim they don't have symptoms and to feel fine when the
diagnosis of hyperparathyroidism is made, almost 100% of parathyroid patients
will actually say they feel better after the parathyroid problem has been
cured--proving they had symptoms. The bottom line: Nearly ALL patients
with parathyroid problems have symptoms. Sometimes the symptoms are real
obvious, like kidney stones, frequent headaches, and depression. Sometimes the
symptoms are not so obvious, like high blood pressure and the inability to
concentrate. If you have symptoms, you are almost guaranteed to feel remarkably
better once the parathyroid tumor has been removed. As we often tell our
parathyroid patients: "you will be amazed at how a 16 minute
mini-procedure will change your life!"
About 95 percent of the
active thyroid hormone is thyroxine, and most of the remaining 5 percent is
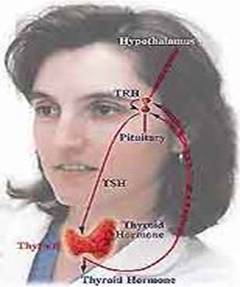
triiodothyronine. Both
of these require iodine for their synthesis. Thyroid hormone secretion is
regulated by a negative feedback mechanism that involves the amount of
circulating hormone, hypothalamus, and adenohypophysis.
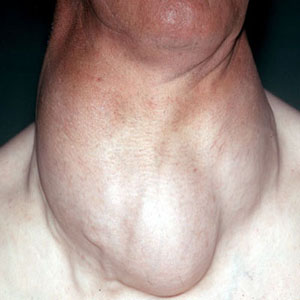
If there is an iodine deficiency, the thyroid cannot make sufficient
hormone. This stimulates the anterior pituitary to secrete thyroid-stimulating
hormone, which causes the thyroid gland to increase in size in a vain attempt
to produce more hormones. But it cannot produce more hormones because it does
not have the necessary raw material, iodine. This type of thyroid enlargement
is called simple goiter or iodine deficiency goiter.

Calcitonin is secreted by the parafollicular cells of the thyroid gland.
This hormone opposes the action of the parathyroid glands by reducing the
calcium level in the blood. If blood calcium becomes too high, calcitonin is
secreted until calcium ion levels decrease to normal.
Calcitonin is a hormone that functions to reduce blood calcium
levels. It is secreted in response to hypercalcemia and has at least two
effects:
- Suppression
of renal tubular reabsorption of calcium. In other words, calcitonin
enhances excretion of calcium into urine.
- Inhibition
of bone resorption, which would minimize fluxes of calcium from bone into
blood.
Although calcitonin has significant calcium-lowing effects in some
species, it appears to have a minimal influence on blood calcium levels in
humans.
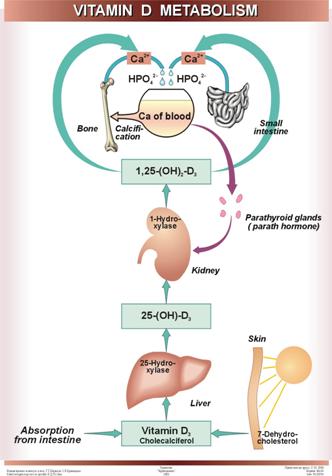
Vitamin D acts also to increase blood concentrations of
calcium. It is
generated through the activity of parathyroid hormone within the kidney. Far
and away the most important effect of vitamin D is to facilitate absorption of
calcium from the small intestine. In concert with parathyroid hormone, vitamin
D also enhances fluxes of calcium out of bone.
http://www.youtube.com/watch?v=JwPVibQ6_3Y&feature=related
http://www.youtube.com/watch?v=n7vybcT9_F4
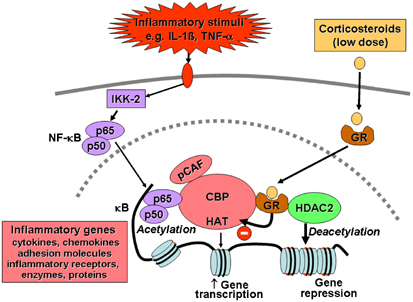
Mechanism of steroid
hormones action (permeating into the cells):
http://www.youtube.com/watch?v=oOj04WsU9ko
In
difference to hormones of protein and peptide nature, receptors for steroid
hormones are located within the cells - in the cytoplasm. From cytoplasm the hormone-receptor
complexes is translocated into the
nucleus where they interact with DNA of nuclear chromatin causing the
activation of genes for respective enzyme proteins. So, if hormones of the
first group cause the activation of existing enzyme molecules, the acting on
the target cells of steroids and thyroid hormones results in the biosynthesis
of new enzyme molecules.
•
Receptors for thyroid
hormones are members of a large family of nuclear receptors that
include those of the steroid hormones. They function as hormone-activated
transcription factors and thereby act by modulating gene expression. In
contrast to steroid hormone receptors, thyroid hormone receptors bind DNA in
the absence of hormone, usually leading to transcriptional repression. Hormone
binding is associated with a conformational change in the receptor that causes
it to function as a transcriptional activator.
•
Currently, four different thyroid hormone receptors are recognized:
alpha-1, alpha-2, beta-1 and beta-2.
•
The presence of multiple forms of the thyroid hormone receptor, with
tissue and stage-dependent differences in their expression, suggests an
extraordinary level of complexity in the physiologic effects of thyroid
hormone.
•
Thyroid hormone receptors bind to short, repeated sequences of DNA
called thyroid or T3 response elements (TREs), a type of hormone
response element. A TRE is composed of two AGGTCA "half sites"
separated by four nucleotides. The half sites of a TRE can be arranged as
direct repeats, pallindromes or inverted repeats.
•
The DNA-binding domain of the receptor contains two sets of four
cysteine residues, and each set chelates a zinc ion, forming loops known as
"zinc fingers". A part of the first zinc finger interacts directly
with nucleotides in the major groove of TRE DNA, while residues in the second
finger interact with nucleotides in the minor groove of the TRE. Thus, the zinc
fingers mediate specificity in binding to TREs.
•
Thyroid hormone receptors can bind to a TRE as monomers, as homodimers
or as heterodimers with the retinoid X receptor (RXR), another member of the
nuclear receptor superfamily that binds 9-cis retinoic acid. The heterodimer
affords the highest affinity binding, and is thought to represent the major
functional form of the receptor.
•
Thyroid hormone receptors bind to TRE DNA regardless of whether they are
occupied by T3.
However, the biological effects of TRE binding by the unoccupied versus the
occupied receptor are dramatically different. In general, binding of thyroid
hormone receptor alone to DNA leads to repression of transcription, whereas
binding of the thyroid hormone-receptor complex activates transcription.
http://www.youtube.com/watch?v=0ss8YIoKw0g
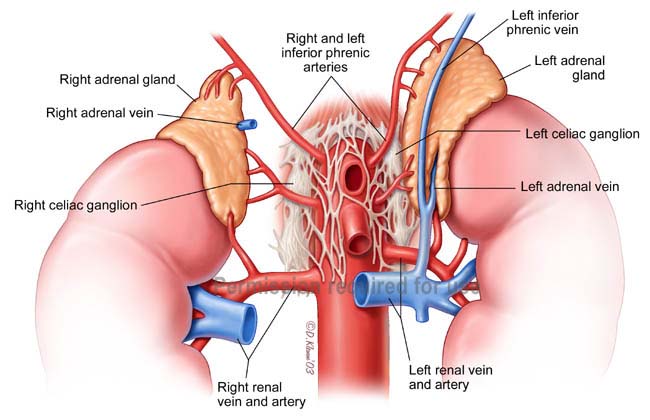
Hormones of adrenal
cortex.
Adrenal glands consist of two parts:
external - cortex, internal - medulla.
Each part secrets specific hormones.
Hormones synthesized in adrenal cortex
are named corticosteroids.
Corticosteroids have potent regulatory effect
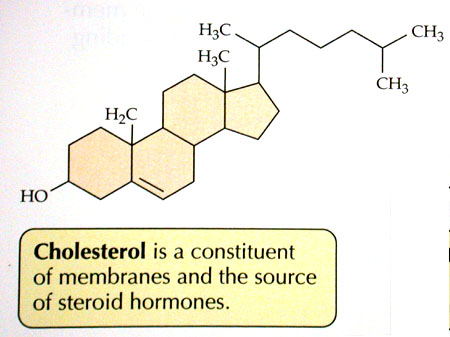
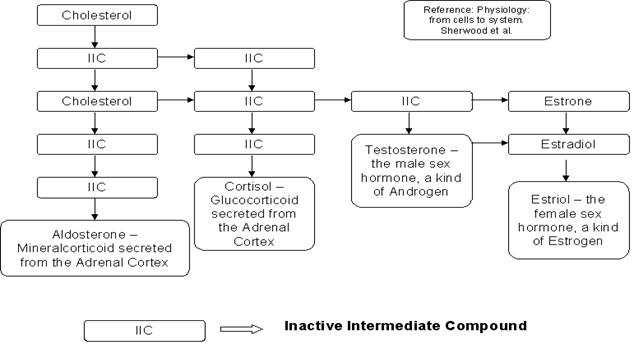
on all kinds of metabolism. Cholesterol is the precursor of corticosteroids.
According to the biological effect corticosteroids are divided on two groups: glucocorticoids and mineralocorticoids. Glucocorticoids regulate the protein,
lipid and carbohydrate metabolism, mineralocorticoids - metabolism of water and
mineral salt.
The most important glucocorticoids: corticosterone, hydrocortisone, cortisol. The most important mineralocorticoid: aldosterone.
All biological active hormones of
adrenal cortex consist of 21 carbon atom and can be reviewed as derivatives of
carbohydrate pregnane.
The synthesis of
corticosteroids is regulated by ACTH.
In the blood corticosteroids are
connected with proteins and transported to different organs.
Time half-life for corticosteroids
is about 1 hour.
Ways of metabolism of
corticosteroids:
1. Reduction. Corticosteroids accept 4
or 6 hydrogen atoms and form couple compounds with glucuronic acid. These
compounds ere excreted by kidneys.
2. Oxidation of 21-st carbon atom.
3. Reduction of ring and decomposition
of side chain. As result 17-ketosteroids are formed that are excreted with urine. The
determination of 17-ketosteroids in urine - important diagnostic indicator.
This is the indicator of adrenal cortex function. In men 17-ketosteroids are
also the terminal products of sex hormones metabolism giving important
information about testicles function.
4. Corticosteroids can be excreted by kidneys in
native structure.
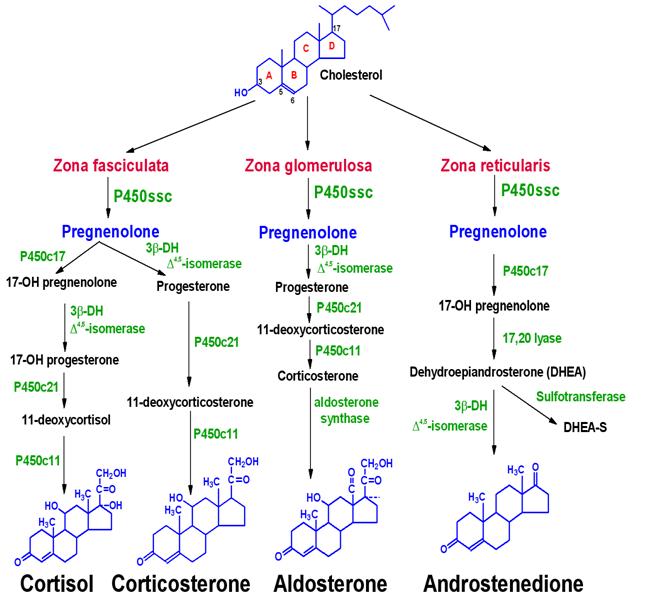
The natural steroid hormones are generally synthesized from cholesterol in the gonads and adrenal glands.
These forms of hormones are lipids.
They can enter the cell membrane quite easily and enter right into the nuclei.
Steroid hormones are generally carried in the blood bound to specific carrier proteins such as
sex hormone binding globulin or corticosteroid binding globulin. Further
conversions and catabolism occurs in the liver, other "peripheral"
tissues, and in the target tissues.
Because steroids and sterols are lipid soluble, they can diffuse fairly
freely from the blood through the cell membrane and
into the cytoplasm of
target cells. In the cytoplasm the steroid may or may not undergo an enzyme-mediated alteration such as
reduction, hydroxylation, or aromatization. In the cytoplasm, the steroid binds
to the specific receptor, a large metalloprotein. Upon steroid binding, many
kinds of steroid receptor dimerizes, two receptor subunits join together
to form one functional DNA-binding unit
that can enter the cell
nucleus. In some of the hormone systems known, the receptor is
associated with a heat shock protein which is released on the binding of the ligand, the hormone. Once in the nucleus,
the steroid-receptor ligand complex binds to specific DNA sequences and induces transcription of
its target genes.
It discussing steroid hormones, one is required to
talk about cholesterol; cholesterol is know as a sterol, which is a natural
product from the steroid nucleus. Cholesterol
is very important, as we learned, in the production of steroid hormones, in
fact they are the precursor for bile acids (bile acids aid in fat digestion),
steroid hormones, and provitamin D (When irradiated by sunlight it changes to
vitamin D3.
Cholesterol,
if we recall, is incorporated into the cell membrane by lipoproteins.There it
plays a role in the regulation of membrane fluidity. It has been stated that cholesterol is probably
responsible for permitting steroid hormones to enter the cell.
Synthesis of steroid hormons
Functions of
glucocorticoids.
http://www.youtube.com/watch?v=0ss8YIoKw0g
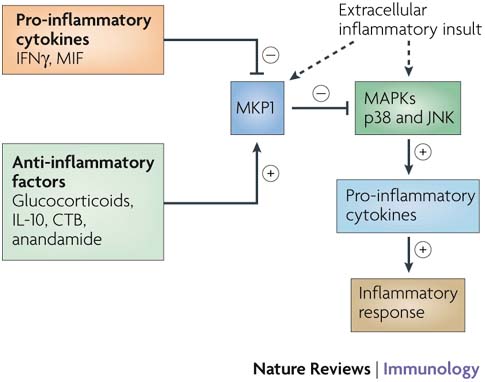
Glucocorticoids have
antiinflammatory, antiallergic, antiimmune
effect. They support the blood pressure and constancy of the
extracellular liquids.
The effect of
glucocorticoids on protein metabolism:
1. stimulate the catabolic processes
(protein decomposition) in connective, lymphoid and muscle tissues and activate
the processes of protein synthesis in liver;
2. stimulate the activity of
aminotransferases;
3. activate the synthesis of urea.
The effect of glucocorticoids on
carbohydrate metabolism:
1. activate the gluconeogenesis;
2. inhibit the activity of hexokinase;
3. activate the glycogen synthesis in
liver.
Glucocorticoids causes the
hyperglycemia.
The effect of
glucocorticoids on lipid metabolism:
1. promote the absorption of lipids in
intestine;
2. activate lipolisis;
3.
activate the conversion of fatty acids in carbohydrates.
Functions of
mineralocorticoids.
Secretion of mineralocorticoids is
regulated by renin-angiotensine system
-
activates the reabsorption of Na+, Cl- and water
in kidney canaliculuses;
-
promote the excretion of K+ by kidneys, skin and saliva.
Deficiency of corticosteroids
causes Addison's disease.
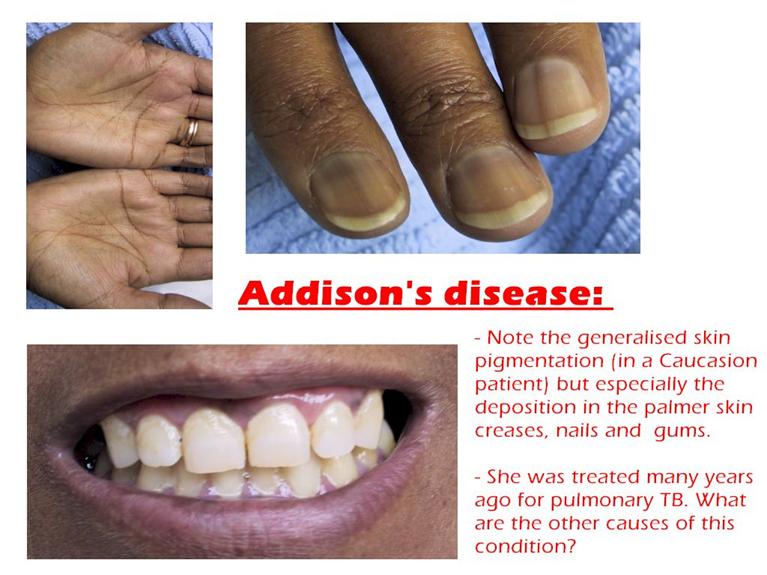
For this disease the
hyperpigmentation is typical because the deficiency of corticosteroids results
in the excessive synthesis of ACTH.
http://www.youtube.com/watch?v=FK1pPqWMXjM
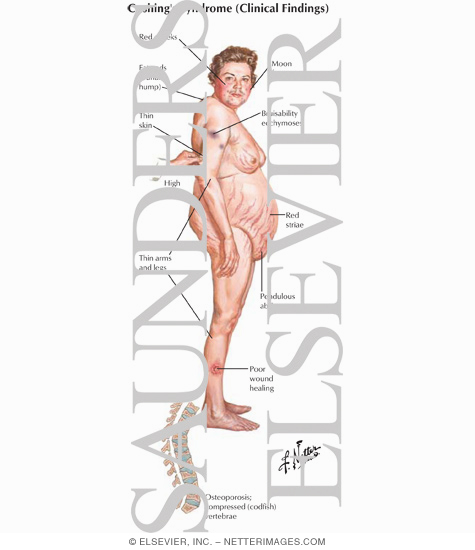
Hyperfunction of adrenal
cortex causes Icenko-Kushing syndrome.
This state is called steroid diabetes. Symptoms: hyperglycemia, glucosuria, hypercholesterolemia,
hypernatriemia, hyperchloremia, hypokaliemia.
http://www.youtube.com/watch?v=ku-QJyQ0j7M&feature=related
hypercholesterolemia
Adrenal cortex hormones
and their artificial analogs are often used in clinic: for treatment of allergic
and autoimmune diseases, in hard shock states.
Blood and urine cortisol, together with the determination of
adrenocorticotropic hormone (ACTH), are the three most important tests in the
investigation of Cushing's syndrome (caused by an overproduction of
cortisol) and Addison's disease (caused by the underproduction of
cortisol).
Cushing's syndrome
Reference ranges for cortisol vary from laboratory to laboratory but are
usually within the following ranges for blood:
- adults
(
- child
one to six years (
- newborn: 1/24 mg/dL.
Reference ranges for cortisol vary from laboratory to laboratory, but are
usually within the following ranges for 24-hour urine collection:
- adult: 10-100 mg/24 hours
- adolescent: 5-55 mg/24 hours
- Child: 2-27 mg/24 hours.
Abnormal results
Increased levels of cortisol are found in Cushing's syndrome, excess
thyroid (hyperthyroidism), obesity, ACTH-producing tumors, and
high levels of stress.

Decreased levels of cortisol are found in Addison's disease, conditions of
low thyroid, and hypopituitarism, in which pituitary activity is
diminished.
Addison's disease
A rare disorder
in which symptoms are caused by a deficiency of hydrocortisone (cortisol) and
aldosterone, two corticosteroid hormones normally produced by a part of the
adrenal glands called the adrenal cortex. Symptoms include weakness, tiredness,
vague abdominal pain, weight loss, skin pigmentation and low blood pressure.
.
Cushing's syndrome
A
hormonal disorder caused by an abnormally high level of corticosteroid
hormones. Symptoms include high blood sugar levels, a moon face, weight gain,
and increased blood pressure
In
![]() Since cortisol production by the
adrenal glands is normally under the control of the pituitary (like the thyroid gland), overproduction
can be caused by a tumor in the pituitary or within the adrenal glands
themselves. When a pituitary tumor secretes too much ACTH (Adrenal Cortical
Tropic Hormone), it simply causes the otherwise normal adrenal glands to
produce too much cortisol. This type of Cushings syndrome is termed
"Cushings Disease" and it is diagnosed like other endocrine disorders
by measuring the appropriateness of hormone production. In this case, serum
cortisol will be elevated, and, serum ACTH will be elevated at the same time.
Since cortisol production by the
adrenal glands is normally under the control of the pituitary (like the thyroid gland), overproduction
can be caused by a tumor in the pituitary or within the adrenal glands
themselves. When a pituitary tumor secretes too much ACTH (Adrenal Cortical
Tropic Hormone), it simply causes the otherwise normal adrenal glands to
produce too much cortisol. This type of Cushings syndrome is termed
"Cushings Disease" and it is diagnosed like other endocrine disorders
by measuring the appropriateness of hormone production. In this case, serum
cortisol will be elevated, and, serum ACTH will be elevated at the same time.
![]() When the adrenal glands develop a
tumor, like any other endocrine gland, they usually produce excess amounts of
the hormone normally produced by these cells. If the adrenal tumor is composed
of cortisol producing cells, excess cortisol will be produced which can be
measured in the blood. Under these conditions, the normal pituitary will sense
the excess cortisol and will stop making ACTH in an attempt to slow the adrenal
down. In this manner, physicians can readily distinguish whether excess
cortisol is the result of a pituitary tumor, or an adrenal tumor.
When the adrenal glands develop a
tumor, like any other endocrine gland, they usually produce excess amounts of
the hormone normally produced by these cells. If the adrenal tumor is composed
of cortisol producing cells, excess cortisol will be produced which can be
measured in the blood. Under these conditions, the normal pituitary will sense
the excess cortisol and will stop making ACTH in an attempt to slow the adrenal
down. In this manner, physicians can readily distinguish whether excess
cortisol is the result of a pituitary tumor, or an adrenal tumor.
![]() Even more rare (but placed here for
completion sake) is when excess ACTH is produced somewhere other than the pituitary.
This is extremely uncommon, but certain lung cancers can make ACTH (we don't
know why) and the patients develop Cushings Syndrome in the same way they do as
if the ACTH was coming from the pituitary.
Even more rare (but placed here for
completion sake) is when excess ACTH is produced somewhere other than the pituitary.
This is extremely uncommon, but certain lung cancers can make ACTH (we don't
know why) and the patients develop Cushings Syndrome in the same way they do as
if the ACTH was coming from the pituitary.
Causes of Cushings
Syndrome
ACTH Dependent (80%)
![]() Pituitary Tumors (60%)
Pituitary Tumors (60%)
![]() Lung Cancers (5%)
Lung Cancers (5%)
ACTH Independent (20%)
![]() Benign Adrenal Tumors (adenoma) (25%)
Benign Adrenal Tumors (adenoma) (25%)

![]() Malignant Adrenal Tumors (adrenal
cell carcinoma) (10%)
Malignant Adrenal Tumors (adrenal
cell carcinoma) (10%)

Testing for Cushings
Syndrome
![]() The most sensitive test to check for
the possibility of this disease is to measure the amount of cortisol
The most sensitive test to check for
the possibility of this disease is to measure the amount of cortisol
excreted in the during during a 24 hour time period.
Cortisol is normally secreted in different amounts during the day and night, so
this test usually will be repeated once or twice to eliminate the variability
which is normally seen. This normal variability is why simply checking the
amount of cortisol in the blood is not a very reliable test. A 24 hour free
cortisol level greater than 100 ug is diagnostic of Cushings syndrome. The
second test which helps confirms this diagnosis is the suppression test which
measures the cortisol secretion following the administration of a powerful
synthetic steroid which will shut down steroid production in everybody with a normal
adrenal gland. Subsequent tests will distinguish whether the disease is due to
an ACTH dependent or independent cause.
![]() Invariably, once the diagnosis is
made, patients will undergo a CT scan (or possibly an MRI or Ultrasound) of the
adrenal glands to look for tumors in one or both of them (more information on adrenal x-ray tests on another page). If the laboratory test suggest a
pituitary origin, a CT or MRI of the brain (and possibly of the chest as well)
will be performed.
Invariably, once the diagnosis is
made, patients will undergo a CT scan (or possibly an MRI or Ultrasound) of the
adrenal glands to look for tumors in one or both of them (more information on adrenal x-ray tests on another page). If the laboratory test suggest a
pituitary origin, a CT or MRI of the brain (and possibly of the chest as well)
will be performed.
Treatment of Cushings
Syndrome
![]() Obviously, the treatment of this
disease depends upon the cause. Pituitary tumors are usually removed surgically
and often treated with radiation therapy. Neurosurgeons and some ENT surgeons
specialize in these tumors. If the cause is determined to be within a single
adrenal gland, this is treated by surgical removal. If the tumor has
characteristics of cancer on any of the x-ray tests, then a larger, conventional
operation is in order. If a single adrenal gland possesses a small, well
defined tumor, it can usually be removed by the new technique of laparoscopic
adrenalectomy.
Obviously, the treatment of this
disease depends upon the cause. Pituitary tumors are usually removed surgically
and often treated with radiation therapy. Neurosurgeons and some ENT surgeons
specialize in these tumors. If the cause is determined to be within a single
adrenal gland, this is treated by surgical removal. If the tumor has
characteristics of cancer on any of the x-ray tests, then a larger, conventional
operation is in order. If a single adrenal gland possesses a small, well
defined tumor, it can usually be removed by the new technique of laparoscopic
adrenalectomy.
Glucocorticoids
Glucocorticoids originate in the adrenal cortex and
affect mainly metabolism in diverse ways; decrease inflammation and increase
resistance to stress.

Mineralocorticoids originate in
adrenal cortex and maintain salt and water balance.
Estrogens originate in the adrenal cortex
and gonads and primarily affect maturation and function of secondary sex organs
(female sexual determination).
Androgens originate in the adrenal
cortex and gonads and primarily affect maturation and function of secondary sex
organs (male sexual determination).
Progestins originate from both
ovaries and placenta, and mediate menstrual cycle and maintain pregnancy.
Androgens and estrogens play a major role in the development of both sexes
secondary characteristics. Androgens, or testosterone and androsterone give the
male its sex characteristics during puberty and for promoting tissue and muscle
growth. Estrogens, or estrone and estradiol are forms of testosterone
synthesized in the ovaries, which control female secondary characteristics and
regulation of the menstrual cycle. Another sex hormone is needed for preparing
the uterus for implantation of the ovum, this hormone is progesterone.
Hormones are needed throughout the body for various functions, however,
just as important as these function is the regulation and control of these
steroids.
http://www.youtube.com/watch?v=nLmg4wSHdxQ&feature=fvwrel
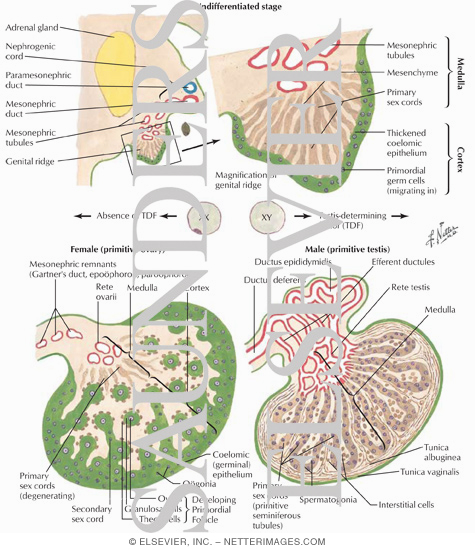
Sex hormones.
Sex hormones are synthesized in
testicles, ovaries. Smaller amount of sex hormones are produced in adrenal
cortex and placenta. Small amount of male sex hormones are produced in ovaries
and female sex hormones - in testicles.
Male sex hormones are called androgens and female - estrogens.
Chemical structure - steroids.
Synthesis and secretion of the sex
hormones are controlled by the pituitary honadotropic hormones. Sex hormones
act by means of the activation of gene apparatus of cells. Catabolism of sex
hormones takes place in liver. The time half-life is 70-90 min.
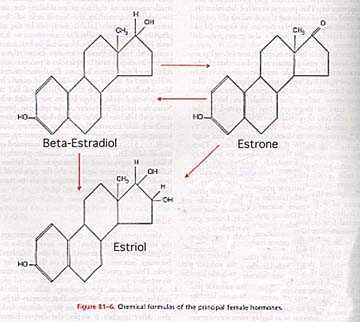
The main estrogens: estradiol,
estrole, estriole (are produced by follicles) and progesterone (is produced
by yellow body and placenta). The main biological role of estrogens -
conditioning for the reproductive female function (possibility of ovum
fertilization). Estradiol results in the proliferation of endometrium and
progesterone stimulates the conversion of endometrium in decidual tissue which
is ready for ovum implantation. Estrogens also cause the development of
secondary sexual features.
The main androgen is testosterone. Its synthesis is regulated by the luteinizing hormone.
Testosterone forms the secondary sexual features in males.
Effect of sex hormones on
protein metabolism:
1. stimulate the processes of protein,
DNA, RNA synthesis;
2. cause the positive nitrogenous
equilibrium.
Effect of sex hormones on carbohydrate
metabolism:
1. activate the Krebs cycle;
2. activate the synthesis of glycogen
in liver.
Effect of sex hormones on
lipid metabolism:
1. enhance the oxidation of lipids;
2. inhibit the synthesis of
cholesterol.
Effect of sex hormones on
energy metabolism:
-
stimulate the Krebs cycle, tissue respiration and ATP production.
Sex hormones are used for treatment of
variety diseases. For example, testosterone and its analogs are used as
anabolic remedies; male sex hormones are used for the treatment of malignant
tumor of female sex organs and vice versa.
Tissue hormones.
Prostaglandins. The precursor of prostaglandins is arachidonic acid.
Time half-life - 30 s. There are different prostaglandins and they have a lot
of physiological and pharmacological effects and different prostaglandins have
different effects.
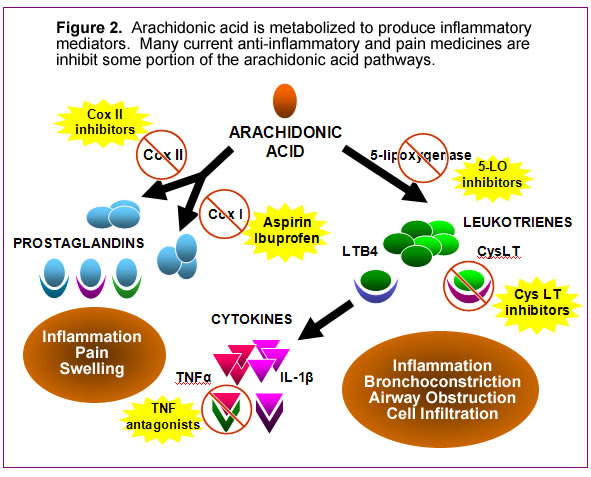
Prostaglandins: - decrease the
activity of lipid tissue lipase;
-
regulate the calcium metabolism in muscle tissue and as result effect on
the contraction and relaxation of muscles;
-
inhibit the gastric secretion;
-
stimulate the formation of steroids.
Kallicrein-kinin system. Kinins -
group of peptides with similar structure and biological properties. The main kinins - bradykinin
and kallidine.
Kinins are formed from their
precursors kininogens that are
synthesized in liver owing to acting of kallicreins. Kallicreins are also
formed from inactive precursors prekallicreins by means of proteolysis.
Functions: - kinins relax the smooth
muscles of blood vessels and decrease the blood pressure;
-
increase the capillaries permeability;
-
takes part in the inflammatory processes.
Renin-angiotensin system. Renin - enzyme
that is synthesized in special cells located near the renal glomerules.
Renin acts on angiotensinogen. As result angiotensin-I
is formed. Under the effect of peptidase
angiotensin-I is converted to angiotensin-II.
Angiotensin-II causes 2 effects:
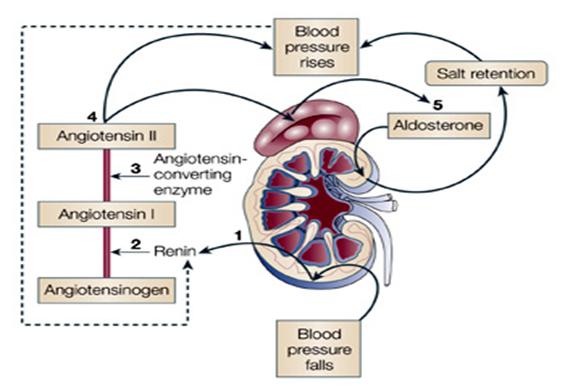
-
narrows the vessels and increases the blood pressure;
-
stimulates the secretion of aldosterone.
The decrease of renal blood stream
is the specific stimulant for renin secretion.
References:
1.
John Mc Murry, Mary E. Castellion. General, Organic
and Biological Chemistry.- New Jersy: Prentice Hall, 1992.- 764 p.
2.
John W. Suttie. Introduction to Biochemistry. – New
York: Holt, Rinehart and Winston, Inc., 1992.- 364 p.
3.
Robert K. Murray, Daryl K. Granner. Harper’s
illustrated Biochemistry. – India: International Education, 2003.- 693 p.
4.
VK Malhotra. Biochemistry for students. – India: Jaypee Brothers,
Medical Publishers LTD, 1998. – 334p.
5. Lehninger A. Principles of
Biochemistry. – New York: Worth Publishers, Inc., 1982. – 1010 p.
6. Stryer L. Biochemistry. – New York:
W.H.Freeman and Company, 1988. – 1086 p.