LESSON 13
Nasal
cavity, larynx.
Trachea,
bronchi, lungs
ORGANIZATION OF THE
RESPIRATORY SYSTEM
We can divide the
respiratory system (Figure 23-1![]() )
) ![]() into an upper respiratory system and a lower
respiratory system. The upper respiratory system consists of the nose,
nasal cavity, paranasal sinuses, and pharynx. These passageways filter, warm,
and humidify the incoming air--protecting the more delicate surfaces of the
lower respiratory system--and cool and dehumidify outgoing air. The lower
respiratory system includes the larynx (voice box), trachea (windpipe),
bronchi, bronchioles, and alveoli of the lungs.
into an upper respiratory system and a lower
respiratory system. The upper respiratory system consists of the nose,
nasal cavity, paranasal sinuses, and pharynx. These passageways filter, warm,
and humidify the incoming air--protecting the more delicate surfaces of the
lower respiratory system--and cool and dehumidify outgoing air. The lower
respiratory system includes the larynx (voice box), trachea (windpipe),
bronchi, bronchioles, and alveoli of the lungs.

Your respiratory
tract consists of the airways that carry air to and from the exchange surfaces
of your lungs. The respiratory tract can be divided into a conducting
portion and a respiratory portion. The conducting portion begins at
the entrance to the nasal cavity and extends through the pharynx and larynx and
along the trachea, bronchi, and bronchioles to the terminal bronchioles.
The respiratory portion of the tract includes the delicate respiratory
bronchioles and the sites of gas exchange, the alveoli.
Filtering,
warming, and humidification of the inspired air begin at the entrance to the
upper respiratory system and continue throughout the rest of the conducting
system. By the time air reaches the alveoli, most foreign particles and
pathogens have been removed, and the humidity and temperature are within
acceptable limits. The success of this "conditioning process" is due
primarily to the properties of the respiratory mucosa.
The Respiratory Mucosa
The respiratory
mucosa lines the conducting portion of the respiratory system. A mucosa is a mucous membrane, one of the four types of
membranes introduced in Chapter 4. It consists of an epithelium and an
underlying layer of loose connective tissue. ![]()
The Respiratory Epithelium ![]()
A
pseudostratified, ciliated, columnar epithelium with numerous goblet cells
(Figure 23-2![]() ) lines the nasal cavity and the superior portion of
the pharynx.
) lines the nasal cavity and the superior portion of
the pharynx. ![]() The structure of the respiratory epithelium changes as
you proceed along the respiratory tract. The epithelium lining inferior
portions of the pharynx is a stratified squamous epithelium similar to that of
the oral cavity. These portions of the pharynx, which conduct air to the lower
respiratory tract, also convey food to the esophagus. The pharyngeal epithelium
must therefore provide protection from abrasion and chemical attack.
The structure of the respiratory epithelium changes as
you proceed along the respiratory tract. The epithelium lining inferior
portions of the pharynx is a stratified squamous epithelium similar to that of
the oral cavity. These portions of the pharynx, which conduct air to the lower
respiratory tract, also convey food to the esophagus. The pharyngeal epithelium
must therefore provide protection from abrasion and chemical attack.

At the beginning
of the lower respiratory tract is a pseudostratified ciliated columnar
epithelium comparable to that of the nasal cavity. In the smaller bronchioles,
this pseudostratified epithelium is replaced by a cuboidal epithelium with
scattered cilia. The exchange surfaces of the alveoli are lined by a very
delicate simple squamous epithelium. Other, more specialized cells are
scattered within the alveolar epithelium.
The Lamina Propria
The lamina propria
is the underlying layer of loose connective tissue that supports the
respiratory epithelium. In the upper respiratory system and in the trachea and
bronchi, the lamina propria contains mucous glands that discharge their
secretions onto the epithelial surface. The lamina propria in the conducting
portions of the lower respiratory system contains bundles of smooth muscle
cells. At the level of the bronchioles, the smooth muscles form relatively
thick bands that encircle or spiral around the lumen.
The
Respiratory Defense System
The delicate
exchange surfaces of the respiratory system can be severely damaged if the
inspired air becomes contaminated with debris or pathogens. Such contamination
is prevented by a series of filtration mechanisms that together make up the
respiratory defense system.
Along much of the
length of the respiratory tract, goblet cells in the epithelium and mucous
glands in the lamina propria produce a sticky mucus that bathes exposed
surfaces. In the nasal cavity, cilia sweep that mucus and any trapped debris or
microorganisms toward the pharynx, where it will be swallowed and exposed to
the acids and enzymes of the stomach. In the lower respiratory system, the
cilia also beat toward the pharynx, moving a carpet of mucus toward the pharynx
and cleaning the respiratory surfaces. This process is often described as a mucus
escalator (Figure 23-2b![]() ).
).
Filtration in the
nasal cavity removes virtually all particles larger than about 10 µm from the
inspired air. Smaller particles may be trapped by the mucus of the nasopharynx
or secretions of the pharynx before proceeding farther along the conducting
system. Exposure to unpleasant stimuli, such as noxious vapors, large
quantities of dust and debris, allergens, or pathogens, generally causes a
rapid increase in the rate of mucus production in the nasal cavity and
paranasal sinuses. (The familiar symptoms of the "common cold" result
from the invasion of this respiratory epithelium by any of more than 200
viruses.)
Most particles 1-5
µm in diameter are trapped in the mucus coating the respiratory bronchioles or
in the liquid covering the alveolar surfaces. These areas are outside the
boundaries of the mucus escalator, but the foreign particles can be engulfed by
alveolar macrophages. Most particles smaller than about 0.5 µm remain suspended
in the air.
Large quantities
of airborne particles may overload the respiratory defenses and produce a
variety of illnesses. For example, the presence of irritants in the lining of
the conducting passageways can provoke the formation of abscesses that block
airflow and reduce pulmonary function, and damage to the epithelium in the
affected area may allow irritants to enter the surrounding tissues of the lung.
The irritants then produce local inflammation, and there is a strong link
between airborne irritants and the development of lung cancer.
THE UPPER RESPIRATORY SYSTEM
The upper
respiratory system consists of the nose, nasal cavity, paranasal sinuses, and
pharynx (Figures 23-1![]() and 23-3ab
and 23-3ab![]() , c
, c![]() ).
).

The Nose and Nasal Cavity ![]()
![]()

The nose is the
primary passageway for air entering the respiratory system. Air normally enters
the respiratory system through the paired external nares, or nostrils (Figure 23-3a![]() ), which open into the nasal cavity. The vestibule is the space contained within the
flexible tissues of the nose (Figure 23-3c
), which open into the nasal cavity. The vestibule is the space contained within the
flexible tissues of the nose (Figure 23-3c![]() ). The epithelium of the vestibule contains coarse
hairs that extend across the external nares. Large airborne particles, such as
sand, sawdust, or even insects, are trapped in these hairs and are thereby
prevented from entering the nasal cavity.
). The epithelium of the vestibule contains coarse
hairs that extend across the external nares. Large airborne particles, such as
sand, sawdust, or even insects, are trapped in these hairs and are thereby
prevented from entering the nasal cavity.
The nasal
septum divides the nasal cavity into left and right portions (Figure 23-3b![]() ). The bony portion of the nasal septum is formed by
the fusion of the perpendicular plate of the ethmoid bone and the plate of the
vomer (Figure 7-3d
). The bony portion of the nasal septum is formed by
the fusion of the perpendicular plate of the ethmoid bone and the plate of the
vomer (Figure 7-3d![]() ). The anterior portion of the nasal septum is formed
of hyaline cartilage. This cartilaginous plate supports the bridge, or dorsum
nasi, and apex (tip) of the nose.
). The anterior portion of the nasal septum is formed
of hyaline cartilage. This cartilaginous plate supports the bridge, or dorsum
nasi, and apex (tip) of the nose.
The maxillary,
nasal, frontal, ethmoid, and sphenoid bones form the lateral and superior walls
of the nasal cavity. The mucous secretions produced in the associated paranasal
sinuses, aided by the tears draining through the nasolacrimal ducts, help keep
the surfaces of the nasal cavity moist and clean. The olfactory region,
or superior portion of the nasal cavity, includes the areas lined by olfactory
epithelium: (1) the inferior surface of the cribriform plate, (2) the superior
portion of the nasal septum, and (3) the superior nasal conchae. Receptors in
the olfactory epithelium provide your sense of smell. ![]()
The superior,
middle, and inferior nasal conchae project toward the nasal septum
from the lateral walls of the nasal cavity. ![]()
![]() To pass from the vestibule to the internal nares, air
tends to flow between adjacent conchae, through the superior, middle, and
inferior meatuses (meatus, a passage) (Figure 23-3b
To pass from the vestibule to the internal nares, air
tends to flow between adjacent conchae, through the superior, middle, and
inferior meatuses (meatus, a passage) (Figure 23-3b![]() ). These are narrow grooves rather than open
passageways, and the incoming air bounces off the conchal surfaces and churns
around like a stream flowing over rapids. This turbulence serves a purpose: As
the air eddies and swirls, small airborne particles are likely to come into
contact with the mucus that coats the lining of the nasal cavity. In addition
to promoting filtration, the turbulence allows extra time for warming and humidifying
the incoming air. It also creates eddy currents that bring olfactory stimuli to
the olfactory receptors.
). These are narrow grooves rather than open
passageways, and the incoming air bounces off the conchal surfaces and churns
around like a stream flowing over rapids. This turbulence serves a purpose: As
the air eddies and swirls, small airborne particles are likely to come into
contact with the mucus that coats the lining of the nasal cavity. In addition
to promoting filtration, the turbulence allows extra time for warming and humidifying
the incoming air. It also creates eddy currents that bring olfactory stimuli to
the olfactory receptors.
A bony hard palate, formed by portions of the maxillary and palatine
bones, forms the floor of the nasal cavity and separates the oral and nasal
cavities. A fleshy soft palate extends posterior to the hard palate, marking the
boundary between the superior nasopharynx and the rest of the pharynx. The nasal cavity opens
into the nasopharynx at the internal
nares.
The
Nasal Mucosa
The mucosa of the
nasal cavity prepares the air you breathe for arrival at your lower respiratory
system. Throughout much of the nasal cavity, the lamina propria contains an
abundance of arteries, veins, and capillaries that bring nutrients and water to
the secretory cells. The lamina propria of the nasal conchae also contains an
extensive network of large and highly expandable veins. This extensive
vascularization provides a mechanism for warming and humidifying the incoming
air (as well as for cooling and dehumidifying the outgoing air). As cool, dry
air passes inward over the exposed surfaces of the nasal cavity, the warm
epithelium radiates heat and the water in the mucus evaporates. Air moving from
your nasal cavity to your lungs has been heated almost to body temperature, and
it is nearly saturated with water vapor. This mechanism protects more delicate
respiratory surfaces from chilling or drying out—two potentially disastrous
events. Breathing through your mouth eliminates much of the preliminary
filtration, heating, and humidifying of the inspired air. To avoid alveolar
damage, patients breathing on a respirator, which utilizes a tube to provide
air directly into the trachea, must receive air that has been externally
filtered and humidified.
As air moves out
of the respiratory tract, it again passes across the epithelium of the nasal
cavity. This air is warmer and more humid than the air that enters; it warms the
nasal mucosa, and moisture condenses on the epithelial surfaces. Thus breathing
through your nose also helps prevent heat loss and water loss to your
environment.
The Pharynx
The pharynx is a chamber shared by the digestive and respiratory
systems. It extends between the internal nares and the entrances to the larynx
and esophagus. The curving superior and posterior walls of the pharynx are
closely bound to the axial skeleton, but the lateral walls are flexible and
muscular.
The pharynx is
divided into three regions (Figure 23-3c![]() ): the nasopharynx, the oropharynx, and
the laryngopharynx:
): the nasopharynx, the oropharynx, and
the laryngopharynx:
- The nasopharynx is the superior portion of the
pharynx. It is connected to the posterior portion of the nasal cavity
through the internal nares and is separated from the oral cavity by the
soft palate (Figure 23-3c
 ). The nasopharynx is lined by the same
pseudostratified ciliated columnar epithelium as that in the nasal cavity.
The pharyngeal tonsil is located on the posterior wall of the
nasopharynx; on each side, one of the auditory tubes opens into the
nasopharynx.
). The nasopharynx is lined by the same
pseudostratified ciliated columnar epithelium as that in the nasal cavity.
The pharyngeal tonsil is located on the posterior wall of the
nasopharynx; on each side, one of the auditory tubes opens into the
nasopharynx. 
- The oropharynx (oris, mouth) extends between the soft
palate and the base of the tongue at the level of the hyoid bone. The
posterior portion of the oral cavity communicates directly with the
oropharynx, as does the posterior inferior portion of the nasopharynx. At
the boundary between the nasopharynx and the oropharynx, the epithelium
changes from a pseudostratified columnar epithelium to a stratified
squamous epithelium.
- The narrow laryngopharynx, the inferior portion of the pharynx, includes
that portion of the pharynx that lies between the hyoid bone and the
entrance to the larynx and esophagus (Figure 23-3c). Like the oropharynx, it is lined by a
stratified squamous epithelium that can resist mechanical abrasion,
chemical attack, and pathogenic invasion.
THE LARYNX
Structure of the larynx and trachea. Development,
topography, age peculiarities
The Larynx is
situated in anterior neck area on level IV-VI cervical vertebrae. At the front
infrahyoid muscles of neck cover it. Vessels and nervous bundles and lobes of
thyroid gland lie from sides of larynx. Laryngeal part of pharynx adjoins
behind it.
Larynx
skeleton consists of pair and odd cartilages.
Odd
cartilages:
• Thyroid
cartilage, which consists of right and left plates (lamina dextra et
sinistra), and also has superior horns and inferior horns; the plates converge
forming laryngeal prominence (Adam’s apple);
• Cricoid
cartilage which has anteriorly arch behind - plate of cricoid cartilage;
• Epiglottis
cartilage.

The cartilages of the larynx. Posterior view.
Paired
cartilages:
• Arytenoid
cartilage, which has a base and apex, muscular process and vocal process. These
cartilage lie on plate of cricoid cartilage;
• Corniculate
cartilage lies in aryepiglottic fold on top of arytenoid cartilages;
• Cuneiform
cartilage lies in aryepiglottic fold front of corniculate cartilages.
In
larynx they distinguish such articulations:
• Cricoid-thyroid
joint is between inferior cornu of thyroid cartilage and arch of cricoid
cartilage; in this joint movement is possible around transversal axis;
• Cricoid-arytenoid
joint is situated between base of arytenoid cartilages and plate of cricoid
cartilage. Arytenoid cartilage can rotate slide to meet one another.
Ligaments
of the larynx:
•
Thyro-hyoid membrane, which hangs larynx to hyoid bone;
•
Crico-thyroid ligament;
•
Thyro-epiglottic ligament;
•
Hyoepiglottic ligament;
•
Vestibular ligaments, which are situated over vocal ligaments.

The ligaments of the larynx. Antero-lateral view.
Fibroelastic
membrane the larynx:
·
Elastic cone contains in its superior margin vocal
ligament;
·
Quadrangular membrane,
which is situated over elastic cone and in its inferior margin contains
vestibular ligament.
Fibroelastic
membranes together with laryngeal cartilages form a laryngeal skeleton.
The
laryngeal Muscles subdivide on muscles that narrow/broaden the glottis, muscles
that change tension of vocal ligament.
Constrictors
of the glottis:
·
lateral cricoarytenoid muscle;
·
thyroarytenoid muscle;
·
transverse arytenoid muscle;
·
oblique arytenoid muscles.
Muscles-dilators
of the glottis
• thyro-arytenoid
muscle has thyro-epiglottic part. Action: it raises the epiglottis and
broadens an entrance into larynx and vestibule.
• posterior
cricoid-arytenoid muscle.
Muscles
changing tension of vocal ligament:
• crico-thyroid
muscle stretches a vocal ligament.
• vocal
muscle is situated in thickness of vocal fold and changes an tension degree
of vocal cords.
Laryngeal
cavity has aditus laryngis [entrance], vestibule,
interventricular space, glottis and infraglottic cavity.
Larynx
has true vocal folds and glottis. Larynx begins by entrance
into larynx, which is limited at the front, by epiglottis, behind – by
arytenoid cartilages, and laterally - by arytenoepiglottic folds, where
cuneiform and corniculate tubercles are situated (places of the same name
cartilages). Glottis is a most narrow place in laryngeal cavity; it is
situated between right and left vocal plicae. Laryngeal ventricle is
fissure disposed between vocal and vestibular plicae.
Infraglottic
cavity is inferior broadened part of larynx, which continues
into trachea.
The larynx or organ of voice is placed at the upper part
of the air passage. It is situated between the trachea and the root of the
tongue, at the upper and forepart of the neck, where it presents a considerable
projection in the middle line. It forms the lower part of the anterior wall of
the pharynx, and is covered behind by the mucous lining of that cavity; on
either side of it lie the great vessels of the neck. Its vertical extent
corresponds to the fourth, fifth, and sixth cervical vertebræ, but it is
placed somewhat higher in the female and also during childhood. Symington found
that in infants between six and twelve months of age the tip of the epiglottis
was a little above the level of the fibrocartilage between the odontoid process
and body of the axis, and that between infancy and adult life the larynx
descends for a distance equal to two vertebral bodies and two intervertebral
fibrocartilages. According to Sappey the average measurements of the adult
larynx are as follows:
|
|
In
males. |
In
females. |
|
Length |
|
|
|
Transverse diameter |
|
|
|
Antero-posterior diameter |
|
|
|
Circumference |
|
|
Until puberty the larynx of the male differs little in size from that of
the female. In the female its increase after puberty is only slight; in the
male it undergoes considerable increase; all the cartilages are enlarged and the
thyroid cartilage becomes prominent in the middle line of the neck, while the
length of the rima glottidis is nearly doubled.
The larynx is broad above, where it presents the form of a triangular
box flattened behind and at the sides, and bounded in front by a prominent
vertical ridge. Below, it is narrow and cylindrical. It is composed of
cartilages, which are connected together by ligaments and moved by numerous
muscles. It is lined by mucous membrane continuous above with that of the
pharynx and below with that of the trachea.
The Cartilages of the Larynx (cartilagines laryngis) are
nine in number, three single and three paired, as follows:
Thyroid.
Cricoid.
Two Arytenoid.
Two Corniculate.
Two Cuneiform. Epiglottis
The Thyroid Cartilage (cartilago thyreoidea) is the
largest cartilage of the larynx. It consists of two laminæ the anterior
borders of which are fused with each other at an acute angle in the middle line
of the neck, and form a subcutaneous projection named the laryngeal
prominence (pomum Adami). This prominence is most distinct at its
upper part, and is larger in the male than in the female. Immediately above it
the laminæ are separated by a V-shaped notch, the superior thyroid
notch. The laminæ are irregularly quadrilateral in shape, and their
posterior angles are prolonged into processes termed the superior and inferior
cornua.
The outer surface of each lamina presents an oblique line
which runs downward and forward from the superior thyroid tubercle situated
near the root of the superior cornu, to the inferior thyroid tubercle on the
lower border. This line gives attachment to the Sternothyreoideus,
Thyreohyoideus, and Constrictor pharyngis inferior.
The inner surface is smooth; above and behind, it is slightly
concave and covered by mucous membrane. In front, in the angle formed by the
junction of the laminæ, are attached the stem of the epiglottis, the
ventricular and vocal ligaments, the Thyreoarytænoidei, Thyreoepiglottici
and Vocales muscles, and the thyroepiglottic ligament.
The upper border is concave behind and convex in front; it gives
attachment to the corresponding half of the hyothyroid membrane.
The lower border is concave behind, and nearly straight in front,
the two parts being separated by the inferior thyroid tubercle. A small part of
it in and near the middle line is connected to the cricoid cartilage by the
middle cricothyroid ligament.
The posterior border, thick and rounded, receives the insertions
of the Stylopharyngeus and Pharyngopalatinus. It ends above, in the superior
cornu, and below, in the inferior cornu. The superior cornu is long and
narrow, directed upward, backward, and medialward, and ends in a conical
extremity, which gives attachment to the lateral hyothyroid ligament. The inferior
cornu is short and thick; it is directed downward, with a slight
inclination forward and medialward, and presents, on the medial side of its
tip, a small oval articular facet for articulation with the side of the cricoid
cartilage.
During infancy the laminæ of the thyroid cartilage are joined to
each other by a narrow, lozenge-shaped strip, named the intrathyroid
cartilage. This strip extends from the upper to the lower border of the
cartilage in the middle line, and is distinguished from the laminæ by
being more transparent and more flexible.
The Cricoid Cartilage (cartilago cricoidea) is smaller,
but thicker and stronger than the thyroid, and forms the lower and posterior
parts of the wall of the larynx. It consists of two parts: a posterior
quadrate lamina, and a narrow anterior arch, one-fourth or one-fifth
of the depth of the lamina.
The lamina (lamina cartilaginis cricoideæ; posterior
portion) is deep and broad, and measures from above downward about 2 or
The arch (arcus cartilaginis cricoideæ; anterior portion)
is narrow and convex, and measures vertically from 5 to
On either side, at the junction of the lamina with the arch, is a small
round articular surface, for articulation with the inferior cornu of the
thyroid cartilage.
The lower border of the cricoid cartilage is horizontal, and
connected to the highest ring of the trachea by the cricotracheal ligament.
The upper border runs obliquely upward and backward, owing to the
great depth of the lamina. It gives attachment, in front, to the middle
cricothyroid ligament; at the side, to the conus elasticus and the
Cricoarytænoidei laterales; behind, it presents, in the middle, a shallow
notch, and on either side of this is a smooth, oval, convex surface, directed
upward and lateralward, for articulation with the base of an arytenoid
cartilage.
The inner surface of the cricoid cartilage is smooth, and lined
by mucous membrane.
The Arytenoid Cartilages (cartilagines arytænoideæ)
are two in number, and situated at the upper border of the lamina of the
cricoid cartilage, at the back of the larynx. Each is pyramidal in form, and
has three surfaces, a base, and an apex.
The posterior surface is a triangular, smooth, concave, and gives
attachment to the Arytænoidei obliquus and transversus.
The antero-lateral surface is somewhat convex and rough. On it,
near the apex of the cartilage, is a rounded elevation (colliculus) from
which a ridge (crista arcuata) curves at first backward and then
downward and forward to the vocal process. The lower part of this crest
intervenes between two depressions or foveæ, an upper, triangular,
and a lower oblong in shape; the latter gives attachment to the Vocalis muscle.
The medial surface is narrow, smooth, and flattened, covered by
mucous membrane, and forms the lateral boundary of the intercartilaginous part
of the rima glottidis.
The base of each cartilage is broad, and on it is a concave
smooth surface, for articulation with the cricoid cartilage. Its lateral angle
is short, rounded, and prominent; it projects backward and lateralward, and is
termed the muscular process; it gives insertion to the
Cricoarytænoideus posterior behind, and to the Cricoarytænoideus
lateralis in front. Its anterior angle, also prominent, but more pointed,
projects horizontally forward; it gives attachment to the vocal ligament, and
is called the vocal process.
The apex of each cartilage is pointed, curved backward and
medialward, and surmounted by a small conical, cartilaginous nodule, the corniculate
cartilage.
The Corniculate Cartilages (cartilagines corniculatæ;
cartilages of Santorini) are two small conical nodules consisting of yellow
elastic cartilage, which articulate with the summits of the arytenoid
cartilages and serve to prolong them backward and medialward. They are situated
in the posterior parts of the aryepiglottic folds of mucous membrane, and are
sometimes fused with the arytenoid cartilages.
The Cuneiform Cartilages (cartilagines cuneiformes; cartilages
of Wrisberg) are two small, elongated pieces of yellow elastic cartilage,
placed one on either side, in the aryepiglottic fold, where they give rise to
small whitish elevations on the surface of the mucous membrane, just in front
of the arytenoid cartilages.
The Epiglottis (cartilago epiglottica) is a thin lamella
of fibrocartilage of a yellowish color, shaped like a leaf, and projecting
obliquely upward behind the root of the tongue, in front of the entrance to the
larynx. The free extremity is broad and rounded; the attached part or stem is
long, narrow, and connected by the thyroepiglottic ligament to the angle
formed by the two laminæ of the thyroid cartilage, a short distance below
the superior thyroid notch. The lower part of its anterior surface is connected
to the upper border of the body of the hyoid bone by an elastic ligamentous
band, the hyoepiglottic ligament.
The anterior or lingual surface is curved forward, and
covered on its upper, free part by mucous membrane which is reflected on to the
sides and root of the tongue, forming a median and two lateral glossoepiglottic
folds; the lateral folds are partly attached to the wall of the pharynx.
The depressions between the epiglottis and the root of the tongue, on either
side of the median fold, are named the valleculæ. The lower part
of the anterior surface lies behind the hyoid bone, the hyothyroid membrane,
and upper part of the thyroid cartilage, but is separated from these structures
by a mass of fatty tissue.
The posterior or laryngeal surface is smooth, concave from
side to side, concavo-convex from above downward; its lower part projects
backward as an elevation, the tubercle or cushion. When the
mucous membrane is removed, the surface of the cartilage is seen to be indented
by a number of small pits, in which mucous glands are lodged. To its sides the
aryepiglottic folds are attached.
Structure.—The corniculate and
cuneiform cartilages, the epiglottis, and the apices of the arytenoids at first
consist of hyaline cartilage, but later elastic fibers are deposited in the
matrix, converting them into yellow fibrocartilage, which shows little tendency
to calcification. The thyroid, cricoid, and the greater part of the arytenoids
consist of hyaline cartilage, and become more or less ossified as age advances.
Ossification commences about the twenty-fifth year in the thyroid cartilage,
and somewhat later in the cricoid and arytenoids; by the sixty-fifth year these
cartilages may be completely converted into bone.
Ligaments.—The ligaments of the
larynxare extrinsic, i. e., those connecting the thyroid
cartilage and epiglottis with the hyoid bone, and the cricoid cartilage with
the trachea; and intrinsic, those which connect the several cartilages
of the larynx to each other.
Extrinsic Ligaments.—The ligaments
connecting the thyroid cartilage with the hyoid bone are the hyothyroid
membrane, and a middle and two lateral hyothyroid ligaments.
The Hyothyroid Membrane (membrana hyothyreoidea; thyrohyoid
membrane) is a broad, fibro-elastic layer, attached below to the upper
border of the thyroid cartilage and to the front of its superior cornu, and
above to the upper margin of the posterior surface of the body and greater
cornua of the hyoid bone, thus passing behind the posterior surface of the body
of the hyoid, and being separated from it by a mucous bursa, which facilitates
the upward movement of the larynx during deglutition. Its middle thicker part
is termed the middle hyothyroid ligament (ligamentum hyothyreoideum
medium; middle thyrohyoid ligament), its lateral thinner portions are
pierced by the superior laryngeal vessels and the internal branch of the
superior laryngeal nerve. Its anterior surface is in relation with the
Thyreohyoideus, Sternohyoideus, and Omohyoideus, and with the body of the hyoid
bone.
The Lateral Hyothyroid Ligament (ligamentum hyothyreoideum
laterale; lateral thyrohyoid ligament) is a round elastic cord, which forms
the posterior border of the hyothyroid membrane and passes between the tip of
the superior cornu of the thyroid cartilage and the extremity of the greater
cornu of the hyoid bone. A small cartilaginous nodule (cartilago triticea),
sometimes bony, is frequently found in it.

Ligaments of the larynx. Posterior view.
The Epiglottis is connected with the hyoid bone by an elastic
band, the hyoepiglottic ligament (ligamentum hyoepiglotticum),
which extends from the anterior surface of the epiglottis to the upper border
of the body of the hyoid bone. The glossoepiglottic folds of mucous membrane
(page 1075) may also be considered as extrinsic ligaments of the epiglottis.
The Cricotracheal Ligament (ligamentum cricotracheale)
connects the cricoid cartilage with the first ring of the trachea. It resembles
the fibrous membrane which connects the cartilaginous rings of the trachea to
each other.
Intrinsic Ligaments.—Beneath the mucous
membrane of the larynx is a broad sheet of fibrous tissue containing many
elastic fibers, and termed the elastic membrane of the larynx. It is
subdivided on either side by the interval between the ventricular and vocal
ligaments, the upper portion extends between the arytenoid cartilage and the
epiglottis and is often poorly defined; the lower part is a well-marked
membrane forming, with its fellow of the opposite side, the conus elasticus
which connects the thyroid, cricoid, and arytenoid cartilages to one another.
In addition the joints between the individual cartilages are provided with
ligaments.
The Conus Elasticus (cricothyroid membrane) is composed
mainly of yellow elastic tissue. It consists of an anterior and two lateral
portions. The anterior part or middle cricothyroid ligament (ligamentum
cricothyreoideum medium; central part of cricothyroid membrane) is thick
and strong, narrow above and broad below. It connects together the front parts
of the contiguous margins of the thyroid and cricoid cartilages. It is
overlapped on either side by the Cricothyreoideus, but between these is
subcutaneous; it is crossed horizontally by a small anastomotic arterial arch,
formed by the junction of the two cricothyroid arteries, branches of which
pierce it. The lateral portions are thinner and lie close under the
mucous membrane of the larynx; they extend from the superior border of the
cricoid cartilage to the inferior margin of the vocal ligaments, with which
they are continuous. These ligaments may therefore be regarded as the free
borders of the lateral portions of the conus elasticus, and extend from the
vocal processes of the arytenoid cartilages to the angle of the thyroid
cartilage about midway between its upper and lower borders.
An articular capsule, strengthened posteriorly by a well-marked
fibrous band, encloses the articulation of the inferior cornu of the thyroid
with the cricoid cartilage on either side.
Each arytenoid cartilage is connected to the cricoid by a capsule and a
posterior cricoarytenoid ligament. The capsule (capsula articularis
cricoarytenoidea) is thin and loose, and is attached to the margins of the
articular surfaces. The posterior cricoarytenoid ligament (ligamentum
cricoarytenoideum posterius) extends from the cricoid to the medial and
back part of the base of the arytenoid.
The thyroepiglottic ligament (ligamentum thyreoepiglotticum)
is a long, slender, elastic cord which connects the stem of the epiglottis with
the angle of the thyroid cartilage, immediately beneath the superior thyroid
notch, above the attachment of the ventricular ligaments.
Movements.—The articulation
between the inferior cornu of the thyroid cartilage and the cricoid cartilage
on either side is a diarthrodial one, and permits of rotatory and gliding
movements. The rotatory movement is one in which the cricoid cartilage rotates
upon the inferior cornua of the thyroid cartilage around an axis passing
transversely through both joints. The gliding movement consists in a limited
shifting of the cricoid on the thyroid in different directions.
The articulation between the arytenoid cartilages and the cricoid is
also a diarthrodial one, and permits of two varieties of movement: one is a
rotation of the arytenoid on a vertical axis, whereby the vocal process is
moved lateralward or medialward, and the rima glottidis increased or
diminished; the other is a gliding movement, and allows the arytenoid
cartilages to approach or recede from each other; from the direction and slope
of the articular surfaces lateral gliding is accompanied by a forward and
downward movement. The two movements of gliding and rotation are associated,
the medial gliding being connected with medialward rotation, and the lateral
gliding with lateralward rotation. The posterior cricoarytenoid ligaments limit
the forward movement of the arytenoid cartilages on the cricoid.
Interior of the Larynx—The cavity of the
larynx (cavum laryngis) extends from the laryngeal entrance to the
lower border of the cricoid cartilage where it is continuous with that of the
trachea. It is divided into two parts by the projection of the vocal folds,
between which is a narrow triangular fissure or chink, the rima glottidis.
The portion of the cavity of the larynx above the vocal folds is called the vestibule;
it is wide and triangular in shape, its base or anterior wall presenting,
however, about its center the backward projection of the tubercle of the
epiglottis. It contains the ventricular folds, and between these and the vocal
folds are the ventricles of the larynx. The portion below the vocal
folds is at first of an elliptical form, but lower down it widens out, assumes
a circular form, and is continuous with the tube of the trachea.
The entrance of the larynx is a triangular opening, wide in
front, narrow behind, and sloping obliquely downward and backward. It is
bounded, in front, by the epiglottis; behind, by the apices of the arytenoid
cartilages, the corniculate cartilages, and the interarytenoid notch; and on
either side, by a fold of mucous membrane, enclosing ligamentous and muscular
fibers, stretched between the side of the epiglottis and the apex of the
arytenoid cartilage; this is the aryepiglottic fold, on the posterior
part of the margin of which the cuneiform cartilage forms a more or less
distinct whitish prominence, the cuneiform tubercle.

Sagittal section of the larynx and upper part of the trachea
The Ventricular Folds (plicœ ventriculares; superior or
false vocal cords) are two thick folds of mucous membrane, each enclosing a
narrow band of fibrous tissue, the ventricular ligament which is
attached in front to the angle of the thyroid cartilage immediately below the
attachment of the epiglottis, and behind to the antero-lateral surface of the
arytenoid cartilage, a short distance above the vocal process. The lower border
of this ligament, enclosed in mucous membrane, forms a free crescentic margin,
which constitutes the upper boundary of the ventricle of the larynx.
The Vocal Folds (plicœ vocales; inferior or true vocal
cords) are concerned in the production of sound, and enclose two strong
bands, named the vocal ligaments (ligamenta vocales; inferior
thyroarytenoid). Each ligament consists of a band of yellow elastic tissue,
attached in front to the angle of the thyroid cartilage, and behind to the
vocal process of the arytenoid. Its lower border is continuous with the thin
lateral part of the conus elasticus. Its upper border forms the lower boundary
of the ventricle of the larynx. Laterally, the Vocalis muscle lies parallel
with it. It is covered medially by mucous membrane, which is extremely thin and
closely adherent to its surface.

Coronal section of larynx and upper part of trachea.
The Ventricle of the Larynx (ventriculus laryngis [Morgagnii];
laryngeal sinus) is a fusiform fossa, situated between the ventricular
and vocal folds on either side, and extending nearly their entire length. The
fossa is bounded, above, by the free crescentic edge of the ventricular
fold; below, by the straight margin of the vocal fold; laterally,
by the mucous membrane covering the corresponding Thyreoarytænoideus. The
anterior part of the ventricle leads up by a narrow opening into a cecal pouch
of mucous membrane of variable size called the appendix.
The appendix of the laryngeal ventricle (appendix ventriculi
laryngis; laryngeal saccule) is a membranous sac, placed between the
ventricular fold and the inner surface of the thyroid cartilage, occasionally
extending as far as its upper border or even higher; it is conical in form, and
curved slightly backward. On the surface of its mucous membrane are the
openings of sixty or seventy mucous glands, which are lodged in the submucous
areolar tissue. This sac is enclosed in a fibrous capsule, continuous below
with the ventricular ligament. Its medial surface is covered by a few delicate
muscular fasciculi, which arise from the apex of the arytenoid cartilage
and become lost in the aryepiglottic fold of mucous membrane; laterally it is
separated from the thyroid cartilage by the Thyreoepiglotticus. These muscles
compress the sac, and express the secretion it contains upon the vocal folds to
lubricate their surfaces.

The entrance to the larynx, viewed from behind.
The Rima Glottidis is the elongated fissure or chink between the
vocal folds in front, and the bases and vocal processes of the arytenoid
cartilages behind. It is therefore subdivided into a larger anterior
intramembranous part (glottis vocalis), which measures about
three-fifths of the length of the entire aperture, and a posterior
intercartilaginous part (glottis respiratoria). Posteriorly it is
limited by the mucous membrane passing between the arytenoid cartilages. The
rima glottidis is the narrowest part of the cavity of the larynx, and its level
corresponds with the bases of the arytenoid cartilages. Its length, in the
male, is about

Laryngoscopic view of interior of larynx.)
Muscles.—The muscles of the larynx are extrinsic,
passing between the larynx and parts around—these have been described in the
section on Myology; and intrinsic, confined entirely to the larynx.
The intrinsic muscles are:
Cricothyreoideus.
Cricoarytænoideus lateralis.
Cricoarytænoideus posterior.
Arytænoideus.
Thyroarytænoideus.
The Cricothyreoideus (Cricothyroid) Triangular in form, arises
from the front and lateral part of the cricoid cartilage; its fibers diverge,
and are arranged in two groups. The lower fibers constitute a pars obliqua
and slant backward and lateralward to the anterior border of the inferior cornu;
the anterior fibers, forming a pars recta, run upward, backward, and
lateralward to the posterior part of the lower border of the lamina of the
thyroid cartilage.
The medial borders of the two muscles are separated by a triangular
interval, occupied by the middle cricothyroid ligament.
The Cricoarytænoideus posterior (posterior
cricoarytenoid) (Fig. 958) arises
from the broad depression on the corresponding half of the posterior surface of
the lamina of the cricoid cartilage; its fibers run upward and lateralward, and
converge to be inserted into the back of the muscular process of the
arytenoid cartilage. The uppermost fibers are nearly horizontal, the middle oblique,
and the lowest almost vertical.
The Cricoarytænoideus lateralis (lateral cricoarytenoid)
(Fig. 959) is smaller than the preceding, and of an oblong form. It arises
from the upper border of the arch of the cricoid cartilage, and, passing
obliquely upward and backward, is inserted into the front of the muscular
process of the arytenoid cartilage.

Side view of the larynx, showing muscular attachments.

Muscles of larynx. Posterior view.

Muscles of larynx. Side view. Right lamina of thyroid cartilage removed.
The Arytænoideus is a single muscle, filling up the
posterior concave surfaces of the arytenoid cartilages. It arises from
the posterior surface and lateral border of one arytenoid cartilage, and is
inserted into the corresponding parts of the opposite cartilage. It consists of
oblique and transverse parts. The Arytænoideus obliquus, the more
superficial, forms two fasciculi, which pass from the base of one cartilage to
the apex of the opposite one, and therefore cross each other like the limbs of
the letter X; a few fibers are continued around the lateral margin of the
cartilage, and are prolonged into the aryepiglottic fold; they are sometimes
described as a separate muscle, the Aryepiglotticus. The Arytænoideus
transversus crosses transversely between the two cartilages.
The Thyreoarytænoideus (Thyroarytenoid) is a broad,
thin, muscle which lies parallel with and lateral to the vocal fold, and
supports the wall of the ventricle and its appendix. It arises in front
from the lower half of the angle of the thyroid cartilage, and from the middle
cricothyroid ligament. Its fibers pass backward and lateralward, to be inserted
into the base and anterior surface of the arytenoid cartilage. The lower and
deeper fibers of the muscle can be differentiated as a triangular band which is
inserted into the vocal process of the arytenoid cartilage, and into the
adjacent portion of its anterior surface; it is termed the Vocalis, and
lies parallel with the vocal ligament, to which it is adherent.

Muscles of the larynx, seen from above.
A considerable number of the fibers of the Thyreoarytænoideus are
prolonged into the aryepiglottic fold, where some of them become lost, while
others are continued to the margin of the epiglottis. They have received a
distinctive name, Thyreoepiglotticus, and are sometimes described as a
separate muscle. A few fibers extend along the wall of the ventricle from the
lateral wall of the arytenoid cartilage to the side of the epiglottis and
constitute the Ventricularis muscle.
Actions.—In considering the actions of the
muscles of the larynx, they may be conveniently divided into two groups, vix.:
1. Those which open and close the glottis. 2. Those which regulate the degree
of tension of the vocal folds.
The Cricoarytœnoidei posteriores separate the vocal folds,
and, consequently, open the glottis, by rotating the arytenoid cartilages
outward around a vertical axis passing through the cricoarytenoid joints; so
that their vocal processes and the vocal folds attached to them become widely
separated.
The Cricoarytœnoidei laterales close the glottis by rotating
the arytenoid cartilages inward, so as to approximate their vocal processes.
The Arytœnoideus approximates the arytenoid cartilages, and
thus closes the opening of the glottis, especially at its back part.
The Cricothyreoidei produce tension and elongation of the vocal
folds by drawing up the arch of the cricoid cartilage and tilting back the
upper border of its lamina; the distance between the vocal processes and the
angle of the thyroid is thus increased, and the folds are consequently
elongated.
The Thyreoarytœnoidei, consisting of two parts having
different attachments and different directions, are rather complicated as
regards their action. Their main use is to draw the arytenoid cartilages
forward toward the thyroid, and thus shorten and relax the vocal folds. But,
owing to the connection of the deeper portion with the vocal fold, this part,
if acting separately, is supposed to modify its elasticity and tension, while
the lateral portion rotates the arytenoid cartilage inward, and thus narrows
the rima glottidis by bringing the two vocal folds together.
Mucous Membrane.—The mucous membrane of
the larynx is continuous above with that lining the mouth and pharynx, and is
prolonged through the trachea and bronchi into the lungs. It lines the
posterior surface and the upper part of the anterior surface of the epiglottis,
to which it is closely adherent, and forms the aryepiglottic folds which bound
the entrance of the larynx. It lines the whole of the cavity of the larynx;
forms, by its reduplication, the chief part of the ventricular fold, and, from
the ventricle, is continued into the ventricular appendix. It is then reflected
over the vocal ligament, where it is thin, and very intimately adherent; covers
the inner surface of the conus elasticus and cricoid cartilage; and is
ultimately continuous with the lining membrane of the trachea. The anterior
surface and the upper half of the posterior surface of the epiglottis, the
upper part of the aryepiglottic folds and the vocal folds are covered by
stratified squamous epithelium; all the rest of the laryngeal mucous membrane
is covered by columnar ciliated cells, but patches of stratified squamous
epithelium are found in the mucous membrane above the glottis.
Glands.—The mucous membrane of the larynx
is furnished with numerous mucous secreting glands, the orifices of which are
found in nearly every part; they are very plentiful upon the epiglottis, being
lodged in little pits in its substance; they are also found in large numbers
along the margin of the aryepiglottic fold, in front of the arytenoid
cartilages, where they are termed the arytenoid glands. They exist also
in large numbers in the ventricular appendages. None are found on the free
edges of the vocal folds.
Vessels and Nerves.—The chief arteries
of the larynx are the laryngeal branches derived from the superior and inferior
thyroid. The veins accompany the arteries; those accompanying the
superior laryngeal artery join the superior thyroid vein which opens into the
internal jugular vein; while those accompanying the inferior laryngeal artery
join the inferior thyroid vein which opens into the innominate vein. The lymphatic
vessels consist of two sets, superior and inferior. The former accompany
the superior laryngeal artery and pierce the hyothyroid membrane, to end in the
glands situated near the bifurcation of the common carotid artery. Of the
latter, some pass through the middle cricothyroid ligament and open into a
gland lying in front of that ligament or in front of the upper part of the
trachea, while others pass to the deep cervical glands and to the glands
accompanying the inferior thyroid artery. The nerves are derived from
the internal and external branches of the superior laryngeal nerve, from the
recurrent nerve, and from the sympathetic. The internal laryngeal branch is
almost entirely sensory, but some motor filaments are said to be carried by it
to the Arytænoideus. It enters the larynx by piercing the posterior part
of the hyothyroid membrane above the superior laryngeal vessels, and divides
into a branch which is distributed to both surfaces of the epiglottis, a second
to the aryepiglottic fold, and a third, the largest, which supplies the mucous
membrane over the back of the larynx and communicates with the recurrent nerve.
The external laryngeal branch supplies the Cricothyreoideus. The recurrent
nerve passes upward beneath the lower border of the Constrictor pharyngis
inferior immediately behind the cricothyroid joint. It supplies all the muscles
of the larynx except the Cricothyreoideus, and perhaps a part of the
Arytænoideus. The sensory branches of the laryngeal nerves form
subepithelial plexuses, from which fibers pass to end between the cells
covering the mucous membrane.
Over the posterior surface of the epiglottis, in the aryepiglottic
folds, and less regularly in some other parts, taste-buds, similar to those in
the tongue, are found.
The
TRACHEA is a tube, which consists of 16-20
semicircular cartilages, joint each other by annular ligaments. Last
built by connective tissue with smooth muscular fibres. Behind semi-rings
communicate by each other by membranous tracheal wall. Trachea
(windpipe) extends from VI cervical to V thoracic vertebra, where it ramifies
on two principal bronchi. This place is tracheal bifurcation.
Trachea has cervical part and thoracic part. Cervical part at the front
covered by infrahyoid muscles and isthmus of thyroid gland that accords to the
second-third tracheal ring. Esophagus (gullet) passes behind the trachea. Thoracic
part of trachea is situated in superior mediastinum.

Front view of cartilages of
larynx, trachea
PRINCIPAL
BRONCHI are generated from the bifurcation of trachea and have similar
structure as trachea. Right principal bronchus is wider than left and it
is continuation of trachea by its direction. It consists of 6-8 cartilaginous
semirings. Left principal bronchus is longer and narrower and passes
with angle from trachea than right. It consists of 9-12 cartilaginous
semi-ring. The principal bronchi are the bronchi of first order, the bronchial
tree starts from them. The extraneous things, especially in children, more
frequently get into right principal bronchus.

Transverse section of the
trachea, just above its bifurcation, with a bird’s-eye view of the interior.
Inspired (inhaled)
air leaves the pharynx by passing through the glottis, a narrow opening. The larynx surrounds and protects the glottis. The larynx begins
at the level of vertebra C4 or C5 and ends at the level
of vertebra C6. The larynx is essentially a cylinder whose
incomplete cartilaginous walls are stabilized by ligaments and skeletal muscles
(Figure 23-4a,b,c![]() , d
, d![]() ).
).
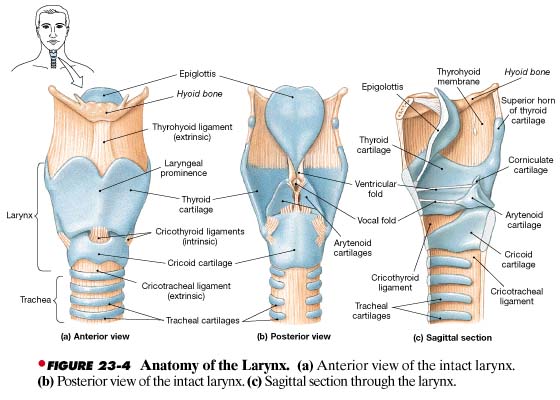
Cartilages of the Larynx
Three large,
unpaired cartilages form the body of the larynx: the thyroid cartilage,
the cricoid cartilage, and the epiglottis (Figure 23-4a,b,c![]() , d
, d![]() ):
):
- The thyroid cartilage (thyroid,
shield-shaped) is the largest laryngeal cartilage. Consisting of hyaline
cartilage, it forms most of the anterior and lateral walls of the larynx.
The thyroid cartilage in section is U-shaped; it is incomplete
posteriorly. The prominent anterior surface of this cartilage, which you
can easily see and feel, is commonly called the Adam's apple. The
inferior surface of the thyroid cartilage articulates with the cricoid
cartilage. The superior surface has ligamentous attachments to the hyoid
bone and to the epiglottis and smaller laryngeal cartilages.
- The thyroid cartilage sits superior to the cricoid (ring-shaped) cartilage, another hyaline
cartilage. The posterior portion of the cricoid is greatly expanded,
providing support in the absence of the thyroid cartilage. The cricoid and
thyroid cartilages protect the glottis and the entrance to the trachea,
and their broad surfaces provide sites for the attachment of important
laryngeal muscles and ligaments. Ligaments attach the inferior surface of
the cricoid cartilage to the first cartilage of the trachea. The superior
surface of the cricoid cartilage articulates with the small, paired arytenoid
cartilages.
- The shoehorn-shaped epiglottis projects superior to the glottis. Composed of
elastic cartilage, it has ligamentous attachments to the anterior and
superior borders of the thyroid cartilage and the hyoid bone. During
swallowing, the larynx is elevated and the epiglottis folds back over the
glottis, preventing the entry of liquids or solid food into the
respiratory passageways.

The larynx also contains
three pairs of smaller hyaline cartilages: the arytenoid, corniculate,
and cuneiform cartilages:
- The arytenoid (ladle-shaped) cartilages articulate with the
superior border of the enlarged portion of the cricoid cartilage.
- The corniculate (horn-shaped) cartilages articulate with the
arytenoid cartilages. The corniculate and arytenoid cartilages are
involved with the opening and closing of the glottis and the production of
sound.
- Elongate, curving cuneiform (wedge-shaped) cartilages lie within folds of
tissue (the aryepiglottic folds) that extend between the lateral
aspect of each arytenoid cartilage and the epiglottis.
Intrinsic
ligaments bind all nine cartilages together to form the larynx (Figure 23-4a,b![]() ). Extrinsic ligaments attach the thyroid cartilage to
the hyoid bone and the cricoid cartilage to the trachea. The ventricular
ligaments and the vocal ligaments extend between the thyroid cartilage and the
arytenoids.
). Extrinsic ligaments attach the thyroid cartilage to
the hyoid bone and the cricoid cartilage to the trachea. The ventricular
ligaments and the vocal ligaments extend between the thyroid cartilage and the
arytenoids.
The ventricular
and vocal ligaments are covered by folds of laryngeal epithelium that project
into the glottis. The ventricular ligaments lie within the superior pair of
folds, known as the ventricular
folds (Figure 23-4b,c![]() , d
, d![]() ). The ventricular folds, which are relatively
inelastic, help prevent foreign objects from entering the glottis and provide
protection for the more delicate vocal folds.
). The ventricular folds, which are relatively
inelastic, help prevent foreign objects from entering the glottis and provide
protection for the more delicate vocal folds.
The vocal folds
guard the entrance to the glottis. They are located inferior to the ventricular
folds. The vocal folds are highly elastic, because they contain bands of
elastic tissue called the vocal ligaments. The vocal folds are involved
with the production of sounds, and for this reason they are known as the true
vocal cords. Because the ventricular folds play no part in sound production,
they are often called the false vocal cords.
Sound
Production
Air passing
through the glottis vibrates the vocal folds and produces sound waves. The
pitch of the sound produced depends on the diameter, length, and tension in the
vocal folds. The diameter and length are directly related to the size of the larynx.
The tension is controlled by the contraction of voluntary muscles that change
the position of the arytenoid cartilages relative to that of the thyroid
cartilage. When the distance increases, the vocal folds tense and the pitch
rises; when the distance decreases, the vocal folds relax and the pitch falls.
Anatomically,
children of both genders have slender, short vocal folds, and their voices tend
to be high-pitched. At puberty, the larynx of a male enlarges considerably more
than that of a female. The true vocal cords of an adult male are thicker and
longer, and they produce lower tones, than those of an adult female.
Sound production
at the larynx is called phonation (phone, voice). Phonation is one component of
speech production, but clear speech also requires articulation, the
modification of those sounds by other structures. In a stringed instrument,
such as a guitar, the quality of the sound produced does not depend solely on
the nature of the vibrating string. The entire instrument becomes involved as
the walls vibrate and the composite sound echoes within the hollow body.
Similar amplification and resonance occur within your pharynx, oral cavity,
nasal cavity, and paranasal sinuses. The combination determines the particular
and distinctive sound of your voice. The final production of distinct words
further depends on voluntary movements of the tongue, lips, and cheeks.
The Laryngeal Musculature
The larynx is
associated with two groups of muscles: (1) the extrinsic laryngeal muscles
and (2) the intrinsic laryngeal muscles. The extrinsic laryngeal
musculature, which includes muscles of the neck and pharynx, positions and
stabilizes the larynx. We considered these muscles in Chapter 11. ![]() The intrinsic laryngeal muscles have two major
functions. One set regulates tension in the vocal folds; a second set opens and
closes the glottis. The muscles involved with the vocal folds insert on the
thyroid, arytenoid, and corniculate cartilages. The opening or closing of the
glottis involves rotational movements of the arytenoids that move the vocal
folds apart or together.
The intrinsic laryngeal muscles have two major
functions. One set regulates tension in the vocal folds; a second set opens and
closes the glottis. The muscles involved with the vocal folds insert on the
thyroid, arytenoid, and corniculate cartilages. The opening or closing of the
glottis involves rotational movements of the arytenoids that move the vocal
folds apart or together.

When you swallow,
both extrinsic and intrinsic muscles cooperate to prevent food or drink from
entering the glottis. Before the material is swallowed, it is crushed and
chewed into a pasty mass known as a bolus. Extrinsic muscles then
elevate the larynx, bending the epiglottis over the entrance to the glottis, so
that the bolus can glide across the epiglottis rather than falling into the
larynx (Figure 23-5![]() ). While this movement is under way, intrinsic muscles
close the glottis. Food particles or liquids that touch the surfaces of the
ventricular or vocal folds will trigger the coughing reflex. In a cough,
the glottis is kept closed while the expiratory muscles contract, elevating
intrapulmonary pressure. When the glottis is opened suddenly, the resulting
blast of air from the trachea generally ejects any material that blocks the
entrance to the glottis.
). While this movement is under way, intrinsic muscles
close the glottis. Food particles or liquids that touch the surfaces of the
ventricular or vocal folds will trigger the coughing reflex. In a cough,
the glottis is kept closed while the expiratory muscles contract, elevating
intrapulmonary pressure. When the glottis is opened suddenly, the resulting
blast of air from the trachea generally ejects any material that blocks the
entrance to the glottis.
CONCEPT CHECK QUESTIONS
- Why is the vascularization of the nasal cavity
important?
- Why is the lining of the nasopharynx different
from that of the oropharynx and laryngopharynx?
- When the tension in your vocal cords increases,
what happens to the pitch of your voice?
THE TRACHEA ![]()
The epithelium of
the larynx is continuous with that of the trachea, or windpipe. The trachea is a tough, flexible tube
with a diameter of about ![]() ). The trachea begins anterior to vertebra C6
in a ligamentous attachment to the cricoid cartilage. It ends in the
mediastinum, at the level of vertebra T5, where it branches to form
the right and left primary bronchi.
). The trachea begins anterior to vertebra C6
in a ligamentous attachment to the cricoid cartilage. It ends in the
mediastinum, at the level of vertebra T5, where it branches to form
the right and left primary bronchi.
The mucosa of the
trachea resembles that of the nasal cavity and nasopharynx. The submucosa, a thick layer of connective tissue, surrounds the
mucosa. The submucosa contains mucous glands that communicate with the
epithelial surface through a number of secretory ducts. The trachea contains
15-20(Figure 23-6a![]() ). Each tracheal cartilage is bound to neighboring
cartilages by elastic annular ligaments. The tracheal cartilages stiffen the
tracheal walls and protect the airway. They also prevent its collapse or
overexpansion as pressures change in the respiratory system.
). Each tracheal cartilage is bound to neighboring
cartilages by elastic annular ligaments. The tracheal cartilages stiffen the
tracheal walls and protect the airway. They also prevent its collapse or
overexpansion as pressures change in the respiratory system.

Each tracheal
cartilage is C-shaped. The closed portion of the C protects the anterior and
lateral surfaces of the trachea. The open portion of the C faces posteriorly,
toward the esophagus. Because the tracheal cartilages do not continue around
the trachea, the posterior tracheal wall can easily distort when you swallow,
permitting the passage of large masses of food through the esophagus.
An elastic
ligament and the trachealis, a band of smooth muscle, connect the ends of each
tracheal cartilage (Figure 23-6b![]() ). Contraction of the trachealis muscle alters the
diameter of the trachea, changing the trachea's resistance to airflow. The
normal diameter of the trachea changes from moment to moment, primarily under
the control of the sympathetic division of the ANS. Sympathetic stimulation
increases the diameter of the trachea and makes it easier to move large volumes
of air along the respiratory passageways.
). Contraction of the trachealis muscle alters the
diameter of the trachea, changing the trachea's resistance to airflow. The
normal diameter of the trachea changes from moment to moment, primarily under
the control of the sympathetic division of the ANS. Sympathetic stimulation
increases the diameter of the trachea and makes it easier to move large volumes
of air along the respiratory passageways.
THE PRIMARY BRONCHI
The trachea
branches within the mediastinum, giving rise to the right and left primary bronchi. A ridge called the carina marks the line of separation between the two bronchi
(Figure 23-6a![]() ). The histological organization of the primary
bronchi is the same as that of the trachea, with cartilaginous C-shaped
supporting rings. The right primary bronchus supplies the right lung, and the
left supplies the left lung. The right primary bronchus is larger in diameter,
and descends toward the lung at a steeper angle, than the left. Thus most
foreign objects that enter the trachea find their way into the right bronchus
rather than the left.
). The histological organization of the primary
bronchi is the same as that of the trachea, with cartilaginous C-shaped
supporting rings. The right primary bronchus supplies the right lung, and the
left supplies the left lung. The right primary bronchus is larger in diameter,
and descends toward the lung at a steeper angle, than the left. Thus most
foreign objects that enter the trachea find their way into the right bronchus
rather than the left.
Before branching
further, each primary bronchus travels to a groove along the medial surface of
its lung. This groove, the hilus of the lung, also provides access for entry to
pulmonary vessels and nerves (Figure 23-![]() ,b
,b![]() ). The entire array is firmly anchored in a meshwork
of dense connective tissue. This complex, known as the root of the lung (Figure
23-6a
). The entire array is firmly anchored in a meshwork
of dense connective tissue. This complex, known as the root of the lung (Figure
23-6a![]() ), attaches to the mediastinum and fixes the positions
of the major nerves, vessels, and lymphatics. The roots of the lungs are
located anterior to vertebrae T5 (right) and T6 (left).
), attaches to the mediastinum and fixes the positions
of the major nerves, vessels, and lymphatics. The roots of the lungs are
located anterior to vertebrae T5 (right) and T6 (left).

THE LUNGS ![]()
![]()
The left and right
lungs (Figure 23-7a![]() , b
, b![]() ) are situated in the left and right pleural cavities.
Each lung is a blunt cone, with the tip, or apex, pointing superiorly. The apex
on each side extends into the base of the neck superior to the first rib. The
broad concave inferior portion, or base, of each lung rests on the superior
surface of the diaphragm.
) are situated in the left and right pleural cavities.
Each lung is a blunt cone, with the tip, or apex, pointing superiorly. The apex
on each side extends into the base of the neck superior to the first rib. The
broad concave inferior portion, or base, of each lung rests on the superior
surface of the diaphragm.

Lobes and Surfaces of the Lungs
The lungs have
distinct lobes separated by deep fissures (Figures 23-7a![]() ,b
,b![]() ). The right lung has three lobes: superior,
middle, and inferior, separated by the horizontal and oblique
fissures. The left lung has only two lobes: superior and inferior,
separated by the oblique fissure. The right lung is broader than the
left, because most of the heart and great vessels project into the left
thoracic cavity. However, the left lung is longer than the right lung, because
the diaphragm rises on the right side to accommodate the mass of the liver.
). The right lung has three lobes: superior,
middle, and inferior, separated by the horizontal and oblique
fissures. The left lung has only two lobes: superior and inferior,
separated by the oblique fissure. The right lung is broader than the
left, because most of the heart and great vessels project into the left
thoracic cavity. However, the left lung is longer than the right lung, because
the diaphragm rises on the right side to accommodate the mass of the liver.
The curving
anterior portion of the lung that follows the inner contours of the rib cage is
the costal surface. The mediastinal surface, containing the hilus, has a more
irregular shape. The mediastinal surfaces of both lungs bear grooves that mark
the passage of the great vessels and of the cardiac impressions, concavities
that conform to the shape of the pericardium (Figures 23-7a![]() ,b
,b![]() and 23-8
and 23-8![]() ). The cardiac impression of the left lung is deeper
than that of the right lung. In anterior view, the medial edge of the right
lung forms a vertical line, whereas the margin of the left lung is indented at
the cardiac notch.
). The cardiac impression of the left lung is deeper
than that of the right lung. In anterior view, the medial edge of the right
lung forms a vertical line, whereas the margin of the left lung is indented at
the cardiac notch.
The Bronchi
The primary
bronchi and their branches form the bronchial tree.![]() Because the left and right primary bronchi are
outside the lungs, they are also called extrapulmonary bronchi. As the primary
bronchi enter the lungs, they divide to form smaller passageways (Figures 23-6
Because the left and right primary bronchi are
outside the lungs, they are also called extrapulmonary bronchi. As the primary
bronchi enter the lungs, they divide to form smaller passageways (Figures 23-6![]() and 23-10a
and 23-10a![]() ). Those branches are collectively called the
intrapulmonary bronchi.
). Those branches are collectively called the
intrapulmonary bronchi.

Each primary
bronchus divides to form secondary bronchi, also known as lobar bronchi. The
right lung has three lobes, and the right primary bronchus divides into three
secondary bronchi: (1) a superior lobar bronchus, (2) a middle lobar
bronchus, and (3) an inferior lobar bronchus. The left lung has two
lobes, and the left primary bronchus divides into two secondary bronchi: (1) a superior
lobar bronchus and (2) an inferior lobar bronchus.
Figure 23-10a![]() follows the branching pattern of the left primary
bronchus as it enters the lung. (The number of branches have been reduced for
clarity.) Within each lung, the secondary bronchi branch to form tertiary
bronchi, or segmental bronchi. The branching pattern differs between the
two lungs, but each tertiary bronchus ultimately supplies air to a single
bronchopulmonary segment,
follows the branching pattern of the left primary
bronchus as it enters the lung. (The number of branches have been reduced for
clarity.) Within each lung, the secondary bronchi branch to form tertiary
bronchi, or segmental bronchi. The branching pattern differs between the
two lungs, but each tertiary bronchus ultimately supplies air to a single
bronchopulmonary segment, ![]()
![]() a specific region of one lung. There are 10
bronchopulmonary segments in the right lung. During development, the left lung
also has 10 segments, but subsequent fusion of adjacent tertiary bronchi
generally reduces that number to eight or nine.
a specific region of one lung. There are 10
bronchopulmonary segments in the right lung. During development, the left lung
also has 10 segments, but subsequent fusion of adjacent tertiary bronchi
generally reduces that number to eight or nine.

The walls of the
primary, secondary, and tertiary bronchi contain progressively lesser amounts
of cartilage. In the secondary and tertiary bronchi, the cartilages form plates
arranged around the lumen. These cartilages serve the same purpose as the rings
of cartilage in the trachea and primary bronchi. As the amount of cartilage
decreases, the relative amount of smooth muscle increases. With less
cartilaginous support, the amount of tension in those smooth muscles has a
greater effect on bronchial diameter and the resistance to airflow.
Each tertiary
bronchus branches several times within the bronchopulmonary segment, giving
rise to multiple bronchioles. These branch further into the finest conducting
branches, called terminal bronchioles. Roughly 6500 terminal bronchioles are
supplied by each tertiary bronchus. Terminal bronchioles have a lumenal
diameter of 0.3-
The walls of
bronchioles, which lack cartilaginous supports, are dominated by smooth muscle
tissue (Figure 23-10b![]() ). In functional terms, the bronchioles are to the
respiratory system what the arterioles are to the cardiovascular system.
Varying the diameter of the bronchioles provides control over the amount of
resistance to airflow and the distribution of air within the lungs.
). In functional terms, the bronchioles are to the
respiratory system what the arterioles are to the cardiovascular system.
Varying the diameter of the bronchioles provides control over the amount of
resistance to airflow and the distribution of air within the lungs.
The ANS regulates
the activity in this smooth muscle layer and thereby controls the diameter of
the bronchioles. Sympathetic activation leads to enlargement of the airway
diameter, or bronchodilation. Parasympathetic stimulation leads to
bronchoconstriction, a reduction in the diameter of the airways.
Bronchoconstriction also occurs during allergic reactions such as anaphylaxis
(Chapter 22), in response to histamine released by activated mast cells and
basophils. ![]()
Bronchodilation
and bronchoconstriction alter the resistance to airflow toward or away from the
respiratory exchange surfaces. Tension in the smooth muscles commonly throws
the bronchiolar mucosa into a series of folds, limiting airflow; excessive
stimulation, as in asthma, can almost completely prevent airflow along
the terminal bronchioles.
Pulmonary Lobules
The connective
tissues of the root of each lung extend into the lung's parenchyma. The fibrous
partitions, or trabeculae, contain elastic fibers, smooth muscles, and lymphatic
vessels. The trabeculae branch repeatedly, dividing the lobes into ever smaller
compartments. The branches of the conducting passageways, pulmonary vessels,
and nerves of the lungs follow these trabeculae. The finest partitions, or
interlobular septa (septum, a wall) divide the lung into pulmonary
lobules, each supplied by branches of the pulmonary arteries, pulmonary veins,
and respiratory passageways (Figure 23-10a![]() , b
, b![]() ). The connective tissues of the septa are in turn
continuous with those of the visceral pleura, the serous membrane
covering the lungs.
). The connective tissues of the septa are in turn
continuous with those of the visceral pleura, the serous membrane
covering the lungs.
Each terminal
bronchiole delivers air to a single pulmonary lobule. Within the lobule, the
terminal bronchiole branches to form several respiratory bronchioles. These are
the thinnest and most delicate branches of the bronchial tree. They deliver air
to the exchange surfaces of the lungs.
The preliminary
filtration and humidification of the incoming air are completed before air
leaves the terminal bronchioles. The epithelial cells of the terminal
bronchioles and respiratory bronchioles are cuboidal, with only scattered
cilia, and there are no goblet cells or underlying mucous glands.
Alveolar Ducts and Alveoli ![]()
Respiratory
bronchioles are connected to individual alveoli and to multiple alveoli along
regions called alveolar ducts (Figures 23-10b![]() ). These passageways end at alveolar sacs, common chambers connected to multiple individual
alveoli. Each lung contains about 150 million alveoli, and their abundance
gives the lung an open, spongy appearance. An extensive network of capillaries
is associated with each alveolus (Figure 23-12a
). These passageways end at alveolar sacs, common chambers connected to multiple individual
alveoli. Each lung contains about 150 million alveoli, and their abundance
gives the lung an open, spongy appearance. An extensive network of capillaries
is associated with each alveolus (Figure 23-12a![]() ); the capillaries are surrounded by a network of
elastic fibers. This elastic tissue helps maintain the relative positions of
the alveoli and respiratory bronchioles. Recoil of these fibers during
exhalation reduces the size of the alveoli and helps push air out of the lungs.
); the capillaries are surrounded by a network of
elastic fibers. This elastic tissue helps maintain the relative positions of
the alveoli and respiratory bronchioles. Recoil of these fibers during
exhalation reduces the size of the alveoli and helps push air out of the lungs.

The Alveolus and the
Respiratory Membrane
The alveolar
epithelium consists primarily of simple squamous epithelium (Figure 23-12b![]() ). The squamous epithelial cells, called Type I
cells, are unusually thin and delicate. Roaming alveolar macrophages (dust
cells) patrol the epithelium, phagocytizing any particulate matter that has
eluded the respiratory defenses and reached the alveolar surfaces. Septal
cells, also called surfactant cells or Type II cells, are scattered
among the squamous cells. These large cells produce an oily secretion, or surfactant, containing a mixture of phospholipids and proteins.
Surfactant is secreted onto the alveolar surfaces, where it forms a superficial
coating over a thin layer of water.
). The squamous epithelial cells, called Type I
cells, are unusually thin and delicate. Roaming alveolar macrophages (dust
cells) patrol the epithelium, phagocytizing any particulate matter that has
eluded the respiratory defenses and reached the alveolar surfaces. Septal
cells, also called surfactant cells or Type II cells, are scattered
among the squamous cells. These large cells produce an oily secretion, or surfactant, containing a mixture of phospholipids and proteins.
Surfactant is secreted onto the alveolar surfaces, where it forms a superficial
coating over a thin layer of water.
Surfactant is
important because it reduces surface tension in the liquid coating the alveolar
surface. As we saw in Chapter 2, surface tension results from the attraction
between water molecules at an air-water boundary. ![]() The alveolar walls are very delicate, and without
surfactant the surface tension would be so high that the alveoli would
collapse. The surfactant forms a thin surface layer that interacts with the
water molecules, reducing the surface tension and keeping the alveoli open.
The alveolar walls are very delicate, and without
surfactant the surface tension would be so high that the alveoli would
collapse. The surfactant forms a thin surface layer that interacts with the
water molecules, reducing the surface tension and keeping the alveoli open.
If surfactant
cells produce inadequate amounts of surfactant due to injury or genetic
abnormalities, the alveoli will collapse, and respiration will become
difficult. On each breath, the inhalation must be forceful enough to pop open
the alveoli. A person with this problem, respiratory distress syndrome,
is soon exhausted by the effort required to keep inflating and deflating the
lungs.
The Respiratory Membrane
Gas exchange occurs across the respiratory membrane of the alveoli. The
respiratory membrane (Figure 23-12c![]() ) is a composite structure consisting of three parts:
) is a composite structure consisting of three parts:
- The squamous epithelial cell lining the alveolus.
- The endothelial cell lining an adjacent
capillary.
- The fused basement membranes that lie between the
alveolar and endothelial cells.

At the respiratory
membrane, the total distance separating the alveolar air and the blood can be
as little as 0.1 µm. Diffusion across the respiratory membrane proceeds very
rapidly, because (1) the distance is small and (2) both oxygen and carbon
dioxide are lipid-soluble. The membranes of the epithelial and endothelial
cells thus do not pose a barrier to the movement of oxygen and carbon dioxide
between the blood and alveolar air spaces.
CONCEPT CHECK QUESTIONS
- Why are the cartilages that reinforce the trachea
C-shaped?
- What would happen to the alveoli if surfactant
were not produced?
- What path does air take in flowing from the
glottis to the respiratory membrane?
The Blood Supply to the Lungs
Your respiratory
exchange surfaces receive blood from arteries of your pulmonary circuit. The
pulmonary arteries enter the lungs at the hilus and branch with the bronchi as
they approach the lobules. Each lobule receives an arteriole and a venule, and
a network of capillaries surrounds each alveolus directly beneath the
respiratory membrane. In addition to providing a mechanism for gas exchange,
the endothelial cells of the alveolar capillaries are the primary source of angiotensin-converting
enzyme (ACE). This enzyme, which converts circulating angiotensin I to
angiotensin II, plays an important role in the regulation of blood volume and
blood pressure (as discussed in Chapters 18 and 21). ![]()
![]()

Blood from the
alveolar capillaries passes through the pulmonary venules and then enters the
pulmonary veins, which deliver it to the left atrium. The conducting portions
of your respiratory tract receive blood from the external carotid arteries
(nasal passages and larynx), the thyrocervical arteries (the inferior larynx
and trachea), and the bronchial arteries (the bronchi and bronchioles).
(See Figures 21-23![]() , 21-24
, 21-24![]() , and 21-26
, and 21-26![]() .) The capillaries supplied by the bronchial arteries
provide oxygen and nutrients to the conducting passageways of your lungs. The
venous blood flows into the pulmonary veins, bypassing the rest of the systemic
circuit and diluting the oxygenated blood leaving the alveoli.
.) The capillaries supplied by the bronchial arteries
provide oxygen and nutrients to the conducting passageways of your lungs. The
venous blood flows into the pulmonary veins, bypassing the rest of the systemic
circuit and diluting the oxygenated blood leaving the alveoli.
THE PLEURAL CAVITIES AND
PLEURAL MEMBRANES
The thoracic
cavity has the shape of a broad cone. Its walls are the rib cage, and the
muscular diaphragm forms the floor. The two pleural cavities are separated by
the mediastinum (Figure 23-8![]() ). Each lung occupies a single pleural cavity, which
is lined by a serous membrane called the pleura (plural, pleurae). The
parietal pleura covers the inner surface of the thoracic wall and extends over
the diaphragm and mediastinum. The visceral pleura covers the outer surfaces of
the lungs, extending into the fissures between the lobes. Each pleural cavity
actually represents a potential space rather than an open chamber, for the
parietal and visceral pleurae are usually in close contact. A small amount of
pleural fluid is secreted by both pleurae. Pleural fluid gives a moist,
slippery coating that provides lubrication, thereby reducing friction between
the parietal and visceral surfaces as you breathe. Samples of pleural fluid,
obtained by means of a long needle inserted between the ribs, are sometimes
obtained for diagnostic purposes. This sampling procedure is called thoracentesis.
The fluid extracted is then examined for the presence of bacteria, blood cells,
or other abnormal components.
). Each lung occupies a single pleural cavity, which
is lined by a serous membrane called the pleura (plural, pleurae). The
parietal pleura covers the inner surface of the thoracic wall and extends over
the diaphragm and mediastinum. The visceral pleura covers the outer surfaces of
the lungs, extending into the fissures between the lobes. Each pleural cavity
actually represents a potential space rather than an open chamber, for the
parietal and visceral pleurae are usually in close contact. A small amount of
pleural fluid is secreted by both pleurae. Pleural fluid gives a moist,
slippery coating that provides lubrication, thereby reducing friction between
the parietal and visceral surfaces as you breathe. Samples of pleural fluid,
obtained by means of a long needle inserted between the ribs, are sometimes
obtained for diagnostic purposes. This sampling procedure is called thoracentesis.
The fluid extracted is then examined for the presence of bacteria, blood cells,
or other abnormal components.

In some disease
states, the normal coating of pleural fluid is unable to prevent friction
between the opposing pleural surfaces. The result is pain and pleural
inflammation, a condition called pleurisy. When pleurisy develops, there may be
excessive secretion of pleural fluid, or the inflamed pleurae may adhere to one
another, limiting relative movement. In either case, breathing becomes
difficult, and prompt medical attention is required.
Changes in the Respiratory System at Birth
There are several
important differences between the respiratory system of a fetus and that of a
newborn infant. Prior to delivery, pulmonary arterial resistance is high, because
the pulmonary vessels are collapsed. The rib cage is compressed, and the lungs
and conducting passageways contain only small amounts of fluid and no air. At
birth, the newborn infant takes a truly heroic first breath through powerful
contractions of the diaphragmatic and external intercostal muscles. The
inspired air must enter the respiratory passageways with enough force to
overcome the surface tension and inflate the bronchial tree and most of the
alveoli. The same drop in pressure that pulls air into the lungs pulls blood
into the pulmonary circulation; the changes in blood flow that occur lead to
the closure of the foramen ovale, an interatrial connection, and the ductus
arteriosus, the fetal connection between the pulmonary trunk and the aorta.
(We detailed these events in Chapters 20 and 21.) ![]()
![]()
The exhalation
that follows fails to empty the lungs completely, for the rib cage does not
return to its former, fully compressed state. Cartilages and connective tissues
keep the conducting passageways open, and the surfactant covering the alveolar
surfaces prevents their collapse. Subsequent breaths complete the inflation of
the alveoli. Pathologists sometimes use these physical changes to determine
whether a newborn infant died before delivery or shortly thereafter. Prior to
the first breath, the lungs are completely filled with fluid, and they will
sink if placed in water. After the infant's first breath, even the collapsed
lungs contain enough air to keep them afloat.
CONCEPT CHECK QUESTIONS
- Which arteries supply blood to the conducting
portions and respiratory exchange surfaces of the lungs?
- What are the functions of the pleura, and what
does it secrete?